

There are a lot of great benefits to a sliding genioplasty chin augmentation procedure but, like all procedures, it has its own unique complications and adverse postoperative sequelae. One of these postoperative issues that can occur is lower lip tightness. Like the upper lip the lower lip is very flexible through the depth of the vestibule and its ability to be easily pulled forward.
But the sliding genioplasty by definition makes its entrance through the vestibule and must transect the origin of the mentalis muscle to reach the bone. While the transected metanlis muscle is out back together and the vestibular mucosa closed it is easy how scar tissue from this process may make the lower lip less flexible. That alone might be enough to cause this postoperative problem but the bony stepoff from an advancement and the increased bone surface area that needs to be covered can be another contributing factor.
While some initial lower lip tightness is to be expected in the healing phase when it fails to adequately resolve in 3 to 4 months after the surgery intervention may be warranted. Non-surgical methods such as steroid, fat or PRP injections can be used. Their effectiveness is not assured and, if they were to work, it would be in the first few months after the surgery. Beyond that it must be treated like a conventional scar contracture with release and grafting.
 A surgical release is the equivalent of opening up the entire bone site almost to the amount that was done to do the original osteotomy. This is necessary if the fixtion plate needs to be removed and such hardware removal is often touted as the treatment for lower lip tightness…but that is rarely effective by itself as the hardware is not really the problem. The real benefit of hardware removal is that it makes the surgeon do an adequate release of the contracted soft tissues.
A surgical release is the equivalent of opening up the entire bone site almost to the amount that was done to do the original osteotomy. This is necessary if the fixtion plate needs to be removed and such hardware removal is often touted as the treatment for lower lip tightness…but that is rarely effective by itself as the hardware is not really the problem. The real benefit of hardware removal is that it makes the surgeon do an adequate release of the contracted soft tissues.
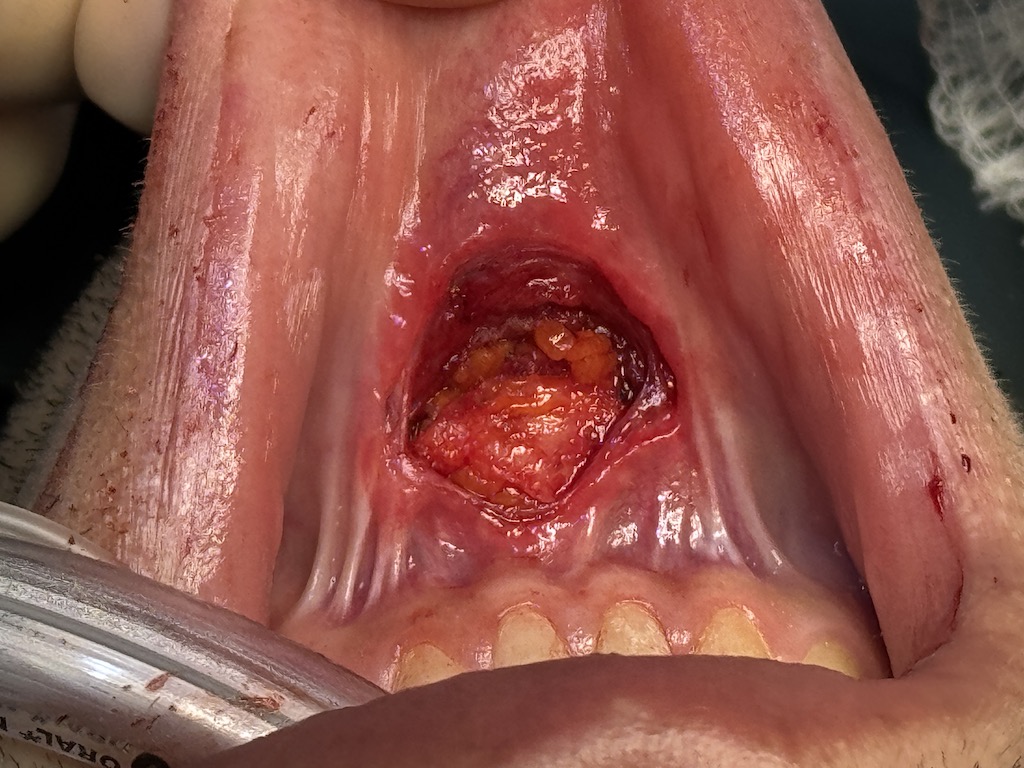
 But the reason a release/hardware removal is not ideally effective is because the release is just half of the solution. A scar contracture really means a soft tissue deficiency. So once the release is done there remains an open or dead space. If it isn’t filled with new supple soft tissue the dead space will close down by filling in with new scar tissue that will likely just tighten back down. A graft is required and the best autologous material is fat. Specifically an enbloc or solid fat graft works best when the volume needed is small. This is the dermal-fat graft whose volume needed is far less than the size of the buccal fat pad. This graft can be harvested from any favorable skin site or even a piece of the buccal fat pad can be used.
But the reason a release/hardware removal is not ideally effective is because the release is just half of the solution. A scar contracture really means a soft tissue deficiency. So once the release is done there remains an open or dead space. If it isn’t filled with new supple soft tissue the dead space will close down by filling in with new scar tissue that will likely just tighten back down. A graft is required and the best autologous material is fat. Specifically an enbloc or solid fat graft works best when the volume needed is small. This is the dermal-fat graft whose volume needed is far less than the size of the buccal fat pad. This graft can be harvested from any favorable skin site or even a piece of the buccal fat pad can be used.
 The dermal-fat graft is prepared by removing the epithelium from the dermis. It is then placed into the released soft tissue site over the osteotomy. The dermal side of the graft is placed against the bone and the muscle layer is closed over it securing it into position. The mucosa is then closed over the muscle layer.
The dermal-fat graft is prepared by removing the epithelium from the dermis. It is then placed into the released soft tissue site over the osteotomy. The dermal side of the graft is placed against the bone and the muscle layer is closed over it securing it into position. The mucosa is then closed over the muscle layer.
In severe lower lip tightness after a sliding genioplasty the introduction of healthy soft tissue in a released scar contracture should result in a reduction of the symptoms. Such fat grafts do survive fairly well with usually greater than 50% or more in volume retention.
Dr. Barry Eppley
World-Renowned Plastic Surgeon