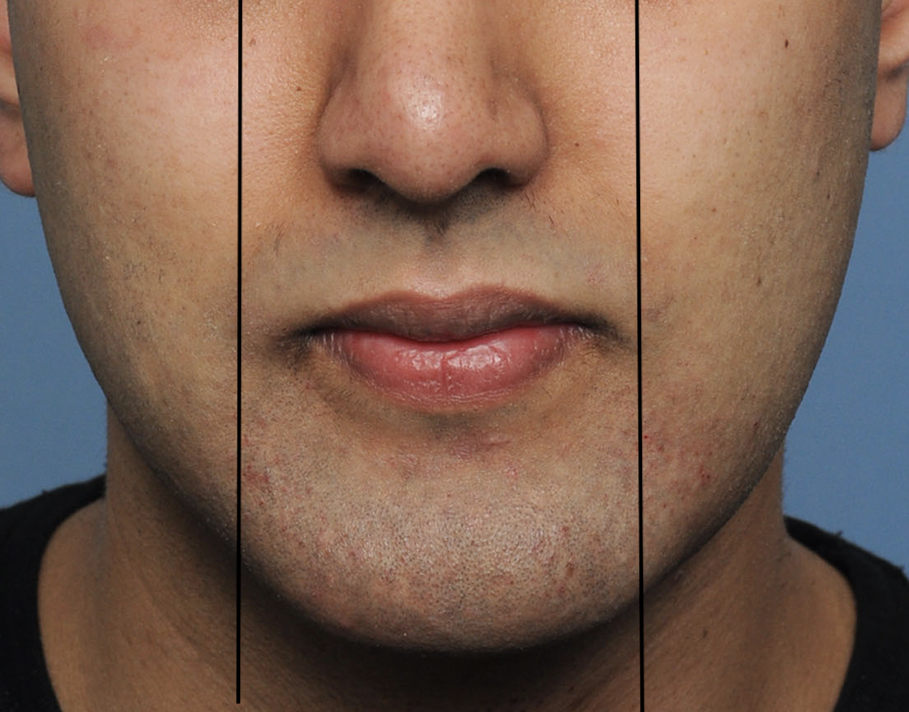


 There are many ratios, angles and linear measurements of the face in assessing proportionate relationships amongst the various facial features. The mouth and lips comprise the distinct features of the lower third of the face in which the lips are a common focus of many aesthetic treatments to improve their size and shape. Once feature of the lips is how wide is the mouth. Most would not think much about mouth size unless it is either too big or too small as defined by the distance between the mouth corners. (commissures) While ultimately the person’s perception of their mouth size is all that aesthetically matters the width of the mouth is defined as being equal to the interpupillary distance. If it is inside these vertical lines it can be considered a small mouth.
There are many ratios, angles and linear measurements of the face in assessing proportionate relationships amongst the various facial features. The mouth and lips comprise the distinct features of the lower third of the face in which the lips are a common focus of many aesthetic treatments to improve their size and shape. Once feature of the lips is how wide is the mouth. Most would not think much about mouth size unless it is either too big or too small as defined by the distance between the mouth corners. (commissures) While ultimately the person’s perception of their mouth size is all that aesthetically matters the width of the mouth is defined as being equal to the interpupillary distance. If it is inside these vertical lines it can be considered a small mouth.
The size of the mouth can be changed with a commissuroplasty procedure. By far the most common direction of aesthetic change is to make a small mouth larger or increase the distance between the mouth corners. This is done by a mouth widening procedure which is done by moving the vermilion edges at the mouth corners.The concept is similar to other forms of vermilion advancement but the vermilion at the mouth corners is different than the rest of the lips. The vermilion show at the mouth corners is very small and the tissue is tight. The mouth corners are also constrained by the orbicularis muscle which envelopes the entire lips but most significantly around the corners in which they have to expand with smiling.



 Successful mouth widening surgery can be done but should be limited to no more than 7mms to avoid undue scarring. Arrow-shaped skin excisions are marked with the maximal widening effect at the tip of the arrow. The tails of the marked excision must go back along the vermilion-cutaneous junction of the upper and lower lip at the mouth corners. This will ensure that the thickness of the vermilion is adequate out to the new mouth corners.
Successful mouth widening surgery can be done but should be limited to no more than 7mms to avoid undue scarring. Arrow-shaped skin excisions are marked with the maximal widening effect at the tip of the arrow. The tails of the marked excision must go back along the vermilion-cutaneous junction of the upper and lower lip at the mouth corners. This will ensure that the thickness of the vermilion is adequate out to the new mouth corners.
Mouth widening surgery is a small procedure but requires attention to detail in performing. It is not quite as simple as removing a segment of skin and the mouth corner just moves out. While the lip vermilion can stretch it won’t go outward willingly and the tendency for relapse is high. A wedge of orbicularis muscle must be removed to give the full thickness of the mouth corners a place to go and where deeper layers can be sutured to support and retain the tissue transposition. This also gives the scars at the mouth corners the best chance to be an acceptable tradeoff.
Dr. Barry Eppley
World-Renowned Plastic Surgeon