

Jaw angle implants are most commonly placed through an intraoral approach without visible external scars. With bilateral posterior vestibular incisions that are up out on the cheek opposite the 2nd molar tooth, subperiosteal dissection is done to elevate the masseter muscle off of the bone. Depending upon the type of jaw angle implant being used, the masseter muscle is elevated just down to the inferior border (widening implant) or onto the bottom edge of the inferior border. (vertical lengthening) Once in proper position it is then secured by screws placed in a percutaneous fashion.
Because of the intraoral approach back in the deeper recesses of the mouth, jaw angle implants have a moderately higher rate of infection (3% to 4%) than other facial implants in my experience. I have used every intraoperative strategy to lower this infection rate but it is just the nature of an intraoral access.
One intraoperative strategy for infection reduction is to change the path of implant insertion to a percutaneous one. While surgeons may be tempted to use the same access to the jaw angles as that used for fracture repair (Risdon incision), this places the scar in a very visible location lower on the neck. And because of its relative remote access, the length of the incision is not short.

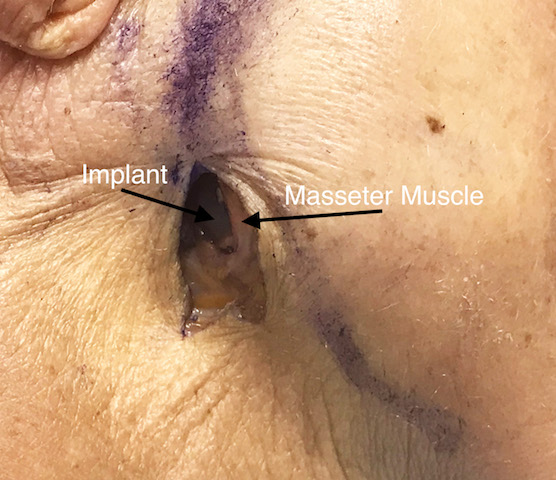
 An alternative but better percutaneous approach is to use a small skin incision right over the jaw angle which provides the most direct access. By placing a 1 to 1.5cm long incision that is curved right at the back side of the bony jaw angle, the masseter muscle and periosteum can be elevated and the pocket created. (cadaver illustrations) By this direct access there is no doubt as to how to position the implant relative to the edges of the bone. The implant can be secured by muscle sutures which also eliminates the risk of masseter muscle dehiscence.
An alternative but better percutaneous approach is to use a small skin incision right over the jaw angle which provides the most direct access. By placing a 1 to 1.5cm long incision that is curved right at the back side of the bony jaw angle, the masseter muscle and periosteum can be elevated and the pocket created. (cadaver illustrations) By this direct access there is no doubt as to how to position the implant relative to the edges of the bone. The implant can be secured by muscle sutures which also eliminates the risk of masseter muscle dehiscence.
This skin incision heals very well with minimal scarring. In most men the incision is usually right at the junction of the beard and non-beard skin. Because it is up at the jaw angle it lies north of the where the marginal mandibular branch of the facial nerve is located.
The percutaneous approach to jaw angle implants lowers the infection risk as well as that of the recovery by eliminating intraoral incisions. Despite these advantages I would still not consider it a first line strategy for most patients. But in those primary or secondary male jaw angle implant placements who are so motivated to avoid intraoral incisions this is a viable incisional technique.
Dr. Barry Eppley
Indianapolis, Indiana