


The sliding genioplasty is one of the most well known chin reshaping procedures. Separating the chin bone by a bone cut done from inside the mouth allows the bone to be moved in a variety of different positions for various chin shape changes. The new position of the chin bone is fixed into position by different types of metal plate and screw techniques.
One of the very important technical steps in the sliding genioplasty procedure is making the bone cut at a level that avoids injury to the inferior alveolar sensory nerve. It has been known for some time based on anatomic studies that the intrabony course of the nerve is lower than where it exits from the bony foramen. This anatomic observation has gone a long way in preventing irreversible numbness to the lip and chin areas from a procedure that has a lot of aesthetic value.
While anatomic studies have been done on the intrabony course of the inferior alveolar nerve, less attention has been paid to its branching pattern through the soft tissues once it leaves the bony foramen. It is known to generally leave the bone in a more upward fashion. But its branching pattern and direction from there have been less well studied.
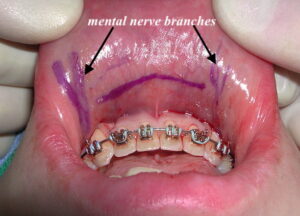 The pertinence of the mental nerve (what the inferior alveolar nerve is called once it leaves the bony foramen) is that some of its branches have the potential to be injured by soft tissue maneuvers in the sliding genioplasty procedure. Anterior branches to come forward which can be cut by long intraoral mucosal incisions. While this results is much less potential for some lower lip numbness than injury at or closer to the main trunk of the nerve, some sensation loss is always possible with any mental branch injury.
The pertinence of the mental nerve (what the inferior alveolar nerve is called once it leaves the bony foramen) is that some of its branches have the potential to be injured by soft tissue maneuvers in the sliding genioplasty procedure. Anterior branches to come forward which can be cut by long intraoral mucosal incisions. While this results is much less potential for some lower lip numbness than injury at or closer to the main trunk of the nerve, some sensation loss is always possible with any mental branch injury.

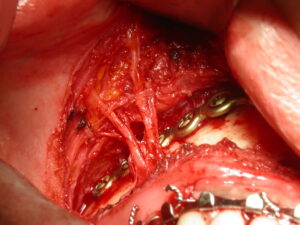
 As a result I have always kept the intraoral incision limited to a length no greater than between the canine teeth. And over the years have evolved to making it even less in length. (between the outer edges of the lateral incisors) The flexibility of the soft tissues allows for the incision to act as a mobile window to perform the bone cuts far to the wide of the chin with full visibility of the mental nerve.
As a result I have always kept the intraoral incision limited to a length no greater than between the canine teeth. And over the years have evolved to making it even less in length. (between the outer edges of the lateral incisors) The flexibility of the soft tissues allows for the incision to act as a mobile window to perform the bone cuts far to the wide of the chin with full visibility of the mental nerve.
 There is also ample access to graft the step off and gaps of the sliding genioplasty with tissue bank coricocancellous bone chips…my graft material of choice in most cases. Closure over the fixation devices and bone chips is done by a two later muscle and mucosal closure that returns to its very small length.
There is also ample access to graft the step off and gaps of the sliding genioplasty with tissue bank coricocancellous bone chips…my graft material of choice in most cases. Closure over the fixation devices and bone chips is done by a two later muscle and mucosal closure that returns to its very small length.
Dr. Barry Eppley
Indianapolis, Indiana