


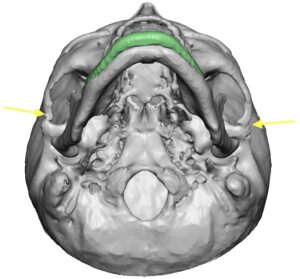
Cheekbone reduction surgery is accomplished by a combination of a front and back osteotomy. (bone cut) The front osteotomy is performed intraorally and cuts through the main body of the cheekbone. The back osteotomy is performed through a skin incision and cuts through the end of the smaller zygomatic arch. The two osteotomies work in tandem to allow the long convex-shaped arch to be moved inward which narrows the face.

 The smaller posterior zygomatic arch osteotomy is unique because of its location and effect. It is performed through an external skin incision directly over the tail of the arch. Through an incision placed at the back side of the sideburn (men) or preauricular hair tuft (women) dissection is done directly down to the bone. This is a facial area where the frontal branch of the facial nerve directly crosses on its way up to the forehead. Most of the time the nerve branch is never encountered and the blunt dissection avoids any risk of nerve injury. But occasionally I have seen it …which actually makes me feel better since I know where it is.
The smaller posterior zygomatic arch osteotomy is unique because of its location and effect. It is performed through an external skin incision directly over the tail of the arch. Through an incision placed at the back side of the sideburn (men) or preauricular hair tuft (women) dissection is done directly down to the bone. This is a facial area where the frontal branch of the facial nerve directly crosses on its way up to the forehead. Most of the time the nerve branch is never encountered and the blunt dissection avoids any risk of nerve injury. But occasionally I have seen it …which actually makes me feel better since I know where it is.

 Once the bone of the zygomatic arch is reached circumferential subperiosteal dissection is done. This both gets around the bone but also allows one to get as far back along the arch at possible. (back to the end of the temporal process of they arch). A reciprocating saw is used to make a full thickness bone cut through the arch. If planning on using plate fixation the bone cut can be done in perpendicular fashion. If no plate fixation is to be used the bone cut is made at an angle. (so the anterior end can be pushed inward and locked behind the posterior end) A four-hole plate is bent so that one hole can be used for screw fixation on each bone end and the intervening 2 holes of the plate in the step off of the cut.
Once the bone of the zygomatic arch is reached circumferential subperiosteal dissection is done. This both gets around the bone but also allows one to get as far back along the arch at possible. (back to the end of the temporal process of they arch). A reciprocating saw is used to make a full thickness bone cut through the arch. If planning on using plate fixation the bone cut can be done in perpendicular fashion. If no plate fixation is to be used the bone cut is made at an angle. (so the anterior end can be pushed inward and locked behind the posterior end) A four-hole plate is bent so that one hole can be used for screw fixation on each bone end and the intervening 2 holes of the plate in the step off of the cut.

 The plate is attached by the two screws which holds the end of the zygomatic arch inward. How much it is moved inward is controlled by the width of the holes in the plate. Two hole widths will equal around 7mms. The skin is then closed with dermal and small resorbable skin sutures. No deeper layers are sutured to avoid potential nerve entrapment.
The plate is attached by the two screws which holds the end of the zygomatic arch inward. How much it is moved inward is controlled by the width of the holes in the plate. Two hole widths will equal around 7mms. The skin is then closed with dermal and small resorbable skin sutures. No deeper layers are sutured to avoid potential nerve entrapment.
 The posterior zygomatic arch osteotomy is most commonly done as part of a total cheekbone reduction. But it can also be done in isolation for the patient who feels their cheek is too wide back closer to their ear. When done by itself the arch will still move inward even though the anterior osteotomy is not done as some bone flexion exists in the thinner arch. It is also possible that the mid-arch suture line can be fractured (greensticked) to help with further posterior arch inward positioning.
The posterior zygomatic arch osteotomy is most commonly done as part of a total cheekbone reduction. But it can also be done in isolation for the patient who feels their cheek is too wide back closer to their ear. When done by itself the arch will still move inward even though the anterior osteotomy is not done as some bone flexion exists in the thinner arch. It is also possible that the mid-arch suture line can be fractured (greensticked) to help with further posterior arch inward positioning.
Dr. Barry Eppley
Indianapolis, Indiana