


Removal or modification of the lower ribcage is based on the premise that it provides structural support to the abdominal wall. This premise is anatomically supported by the numerous attachments of abdominal muscles to the free floating ribs. Ribs #s 11 and 12, also known as the vertebral ribs, have attachments to the anterolateral abdominal wall muscles. These ribs are not attached to the sternum or costal cartilages and, as a result, when the ribs are removed or modified the external waist contour moves inward as the muscles contract.
But the ribs are not the only anatomic structures that helps create the external contour/shape of the waist. There is the skin and subcutaneous fat layer, which can be significant, but in most rib removal candidates they are either thin or have undergone liposuction previously. So these components did not offer much for waist contour change. The one lone remaining structure is the latissimus dorsi (LD) muscle between the subcutaneous fat and the ribs. The outer border of the muscle extends further laterally than the ribs and is quite thick. Removal of some of its thickness at the periumbilical line and above is a helpful adjunct in waist narrowing surgery.

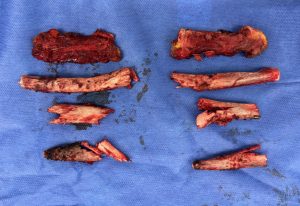
 In traditional Type 1 rib removal surgery the incision location and length permits a wedge of the muscle to be removed. But in Type 2 rib removals the change in incision location and length permits a much greater amount of muscle to be removed vertically. Starting below the lower end of the incision and going as far superiorly as possible above its superior end a 2 to 3m thickness strip of muscle can be removed from its lateral edge.
In traditional Type 1 rib removal surgery the incision location and length permits a wedge of the muscle to be removed. But in Type 2 rib removals the change in incision location and length permits a much greater amount of muscle to be removed vertically. Starting below the lower end of the incision and going as far superiorly as possible above its superior end a 2 to 3m thickness strip of muscle can be removed from its lateral edge.

 The change in the location of the incision to get more muscle and bone removals does not significantly increase the amount of incisional scarring.
The change in the location of the incision to get more muscle and bone removals does not significantly increase the amount of incisional scarring.
Dr. Barry Eppley
World-Renowned Plastic Surgeon