

Iatrogenic ptosis of the soft tissue chin pad can occur for several reasons. The most commons causes are when a chin implant is removed and not replaced or when intraoral chin reduction is done by burring or a setback genioplasty. Correction of the resultant drooping chin pad is done by several different methods of which mentalis muscle resuspension is the most recognized technique.
But the reality is mentalis muscle resuspension rarely works alone. Simply pulling the muscle back up onto the bone seems like it should work but the relapse rate is high. The best results come when the muscle suspension is combined with other procedures particularly some method of chin augmentation. (chin implant or sliding genioplasty) This provides some support for the muscle to hang on to lessening the relapse rate.

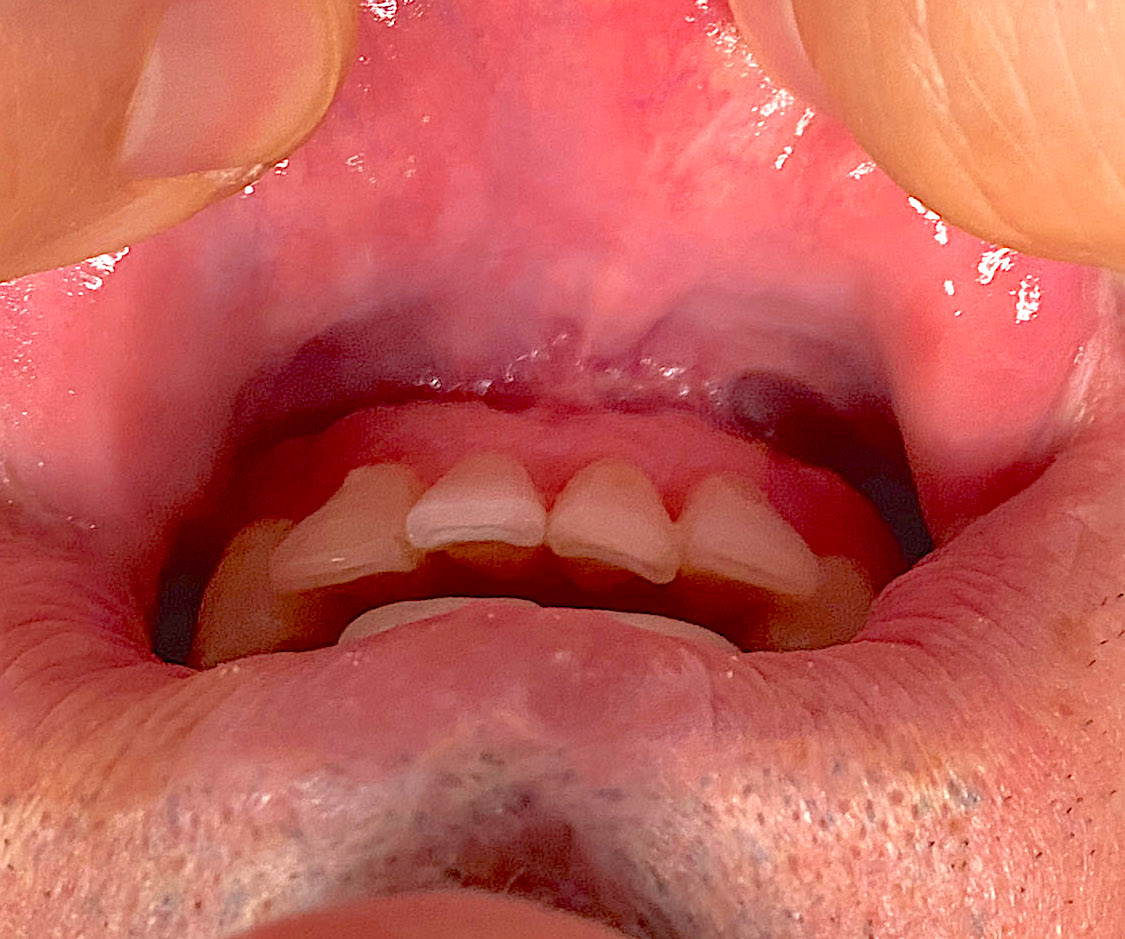
 Another useful technique in the treatment of chin pad ptosis, which is often overlooked, is a shortening vestibuloplasty. In every chin ptosis patient I have seen that also has lower lip incompetence the depth of the vestibule is abnormally deep. The depth of the vestibule is a reflection of the lost muscle attachment to the bone. While muscle suspension and adding chin support are the cornerstones of treatment, shortening the depth of the vestibule is another additive beneficial procedure.
Another useful technique in the treatment of chin pad ptosis, which is often overlooked, is a shortening vestibuloplasty. In every chin ptosis patient I have seen that also has lower lip incompetence the depth of the vestibule is abnormally deep. The depth of the vestibule is a reflection of the lost muscle attachment to the bone. While muscle suspension and adding chin support are the cornerstones of treatment, shortening the depth of the vestibule is another additive beneficial procedure.
 By excising the mucosa of the vestibule between the 1st premolars between the lower lip and lower jaw, the two mucosal edges are sewn together. Its benefit is that it provides support to the elevated lower lip and helps prevent significant relapse. Mucosal closure needs to be done anyways so this additional procedure at the end of the intraoral chin ptosis correction adds no morbidity.
By excising the mucosa of the vestibule between the 1st premolars between the lower lip and lower jaw, the two mucosal edges are sewn together. Its benefit is that it provides support to the elevated lower lip and helps prevent significant relapse. Mucosal closure needs to be done anyways so this additional procedure at the end of the intraoral chin ptosis correction adds no morbidity.
Chin pad ptosis correction is a challenging procedure that is not always 100% assured of a successful outcome. A combination of procedures works best and a shortening vestibuloplasty is another essential component to the chin ptosis correction armentarium.
Dr. Barry Eppley
Indianapolis, Indiana