

For major nasal augmentations the options come to using a rib graft or an implant to achieve it. Each augmentation method has their own advantages and disadvantages and one isn’t necessarily better than the other. Each patient situation must be assessed on an individual basis in terms of amount of augmentation needed and the patient’s risk vs scar tolerance.
The major advantages of a nasal implant are obvious… no donor harvest scar, less operating and recovery time and an assured straight form with a guaranteed augmentation effect based on its dimensions. But one of its known side effects is that the implant can become deviated or misaligned. This risk is greater in silicone nasal implants because they have a smooth surface and contracture around them over time can cause their position to change. This is because they do not integrate into the surrounding tissue and are more prone to deformational forces. Other types of nasal implants, such as porous polyethylene and ePTFE, allow for tissue adherence and are less likely to undergo secondary positional displacement.
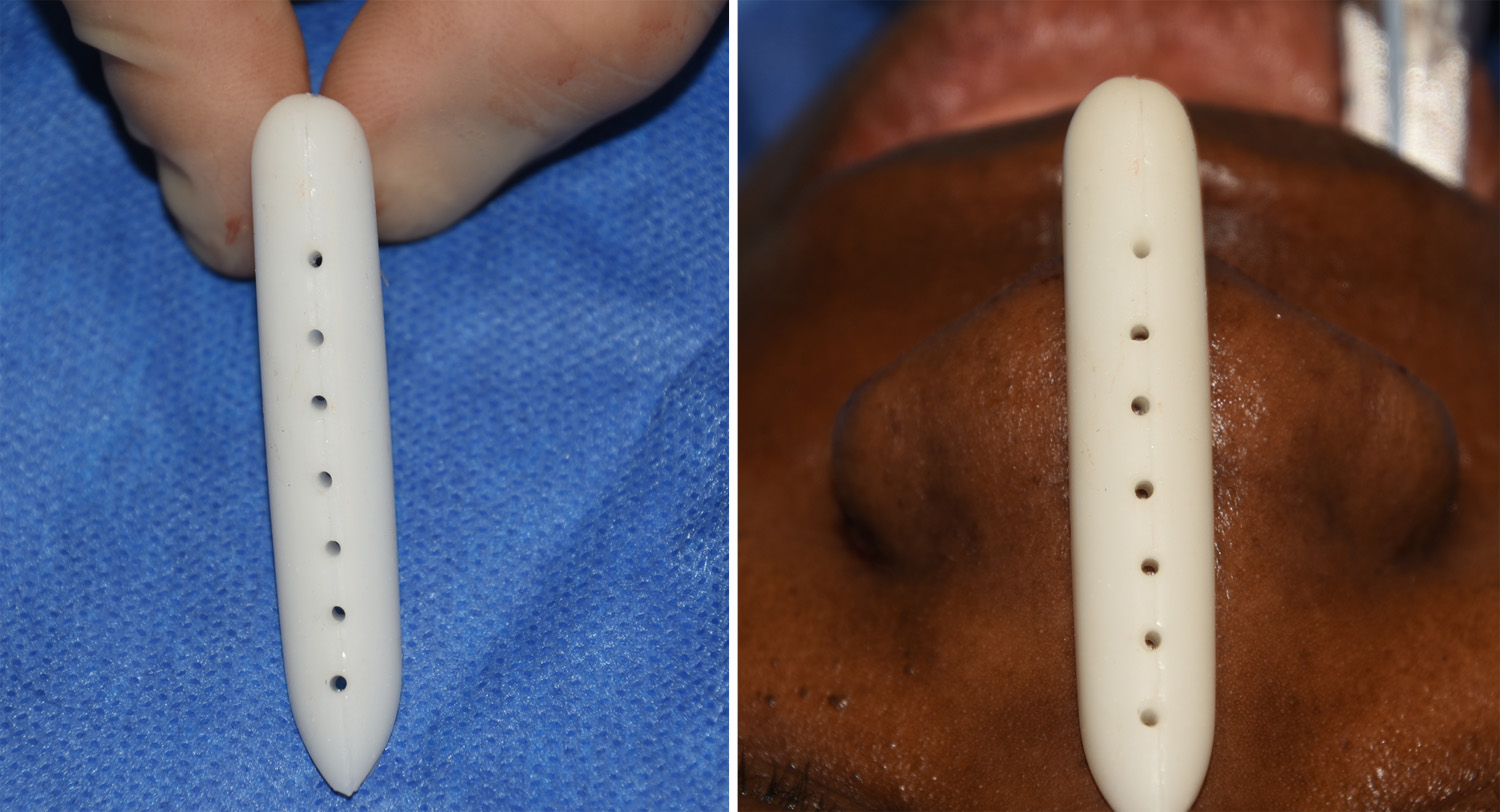 One technique to create some tissue ingrowth into a solid silicone nasal implant is to place perfusion holes. Using a small 2mm dermal punch a series of holes are placed down the middle of the implant. Once implanted tissue will quickly grow into and through the holes to connect the underside of the skin to the perichondrium and periosteum of the nasal bone and cartilage surface. These vertical tunnels of tissue ingrowth serve as individual anchors maintaining the position of the implant regardless of what forces it is exposed to after healing.
One technique to create some tissue ingrowth into a solid silicone nasal implant is to place perfusion holes. Using a small 2mm dermal punch a series of holes are placed down the middle of the implant. Once implanted tissue will quickly grow into and through the holes to connect the underside of the skin to the perichondrium and periosteum of the nasal bone and cartilage surface. These vertical tunnels of tissue ingrowth serve as individual anchors maintaining the position of the implant regardless of what forces it is exposed to after healing.
 While perfusion holes are a useful and simple feature to add to any silicone nasal implant, it is important to respect many other aspects of implantation for a successful long-term outcome. The implant should not be oversized and place too much stress on the overlying tissues, particularly in the tip area. With any portion of the implant near or directly under the nasal tip skin, it needs to have a soft tissue buffer whether it is cartilage, fascia or dermis covering the end of the implant.
While perfusion holes are a useful and simple feature to add to any silicone nasal implant, it is important to respect many other aspects of implantation for a successful long-term outcome. The implant should not be oversized and place too much stress on the overlying tissues, particularly in the tip area. With any portion of the implant near or directly under the nasal tip skin, it needs to have a soft tissue buffer whether it is cartilage, fascia or dermis covering the end of the implant.
Dr. Barry Eppley
Indianapolis, Indiana