

Brow bone reduction is one of numerous types of facial bone reshaping procedures. In its most traditional sense it is done to reduce the horizontal or forward projection of the brow bones. In essence this is to reduce the bulge or outward prominence of them. This is usually done either in men with very large and overgrown frontal sinuses or in male to female transgender surgery to create a perfectly flat brow bone arch. Depending upon the degree of brow bone protrusion and the thickness of the anterior wall of the frontal sinus burring reduction or an osteoplastic bone flap setback procedure can be done.
But excessive brow bone growth or shape can occur in other dimensions as well. Brow bones that are too vertically low or high can cause undesired orbital/eye issues. Brow bones that are too high (increased vertical orbital height) may make the eye look too open and the brows retracted. Brow bones whose edges are too vertically low may make the eye look too closed or push down on the eyelid tissues causing an appearance of eyelid hooding or pseudoptosis.
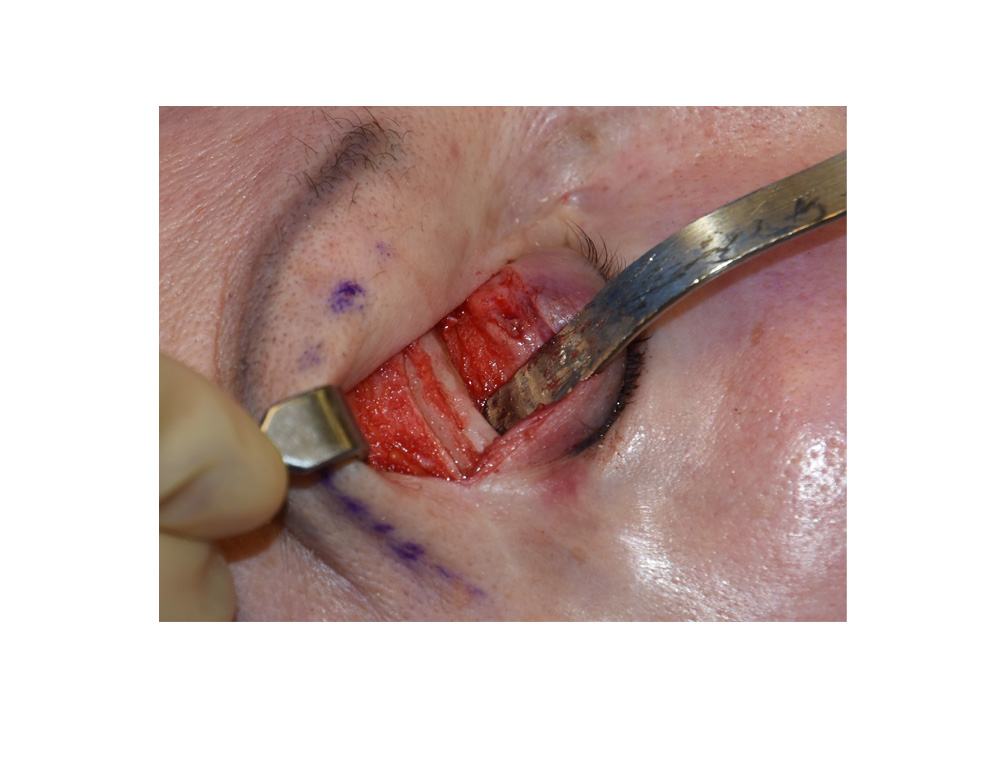 Like horizontal reduction of the brow bones, vertical reduction of them can also be done. This is often combined with horizontal reduction particularly in transgender brow/orbital bone reshaping through a coronal scalp incision. But there are cases when only a vertical brow bone reduction is needed which is usually when it is causing a more ‘closed eye’ appearance or eyelid asymmetry. Rather than using a scalp incision, isolated vertical or tail of the brow bone reduction can be done through an upper eyelid or transpalpebral incisional approach. This direct access allows for a limited dissection technique that more easily isolates the desired brow bone location.
Like horizontal reduction of the brow bones, vertical reduction of them can also be done. This is often combined with horizontal reduction particularly in transgender brow/orbital bone reshaping through a coronal scalp incision. But there are cases when only a vertical brow bone reduction is needed which is usually when it is causing a more ‘closed eye’ appearance or eyelid asymmetry. Rather than using a scalp incision, isolated vertical or tail of the brow bone reduction can be done through an upper eyelid or transpalpebral incisional approach. This direct access allows for a limited dissection technique that more easily isolates the desired brow bone location.
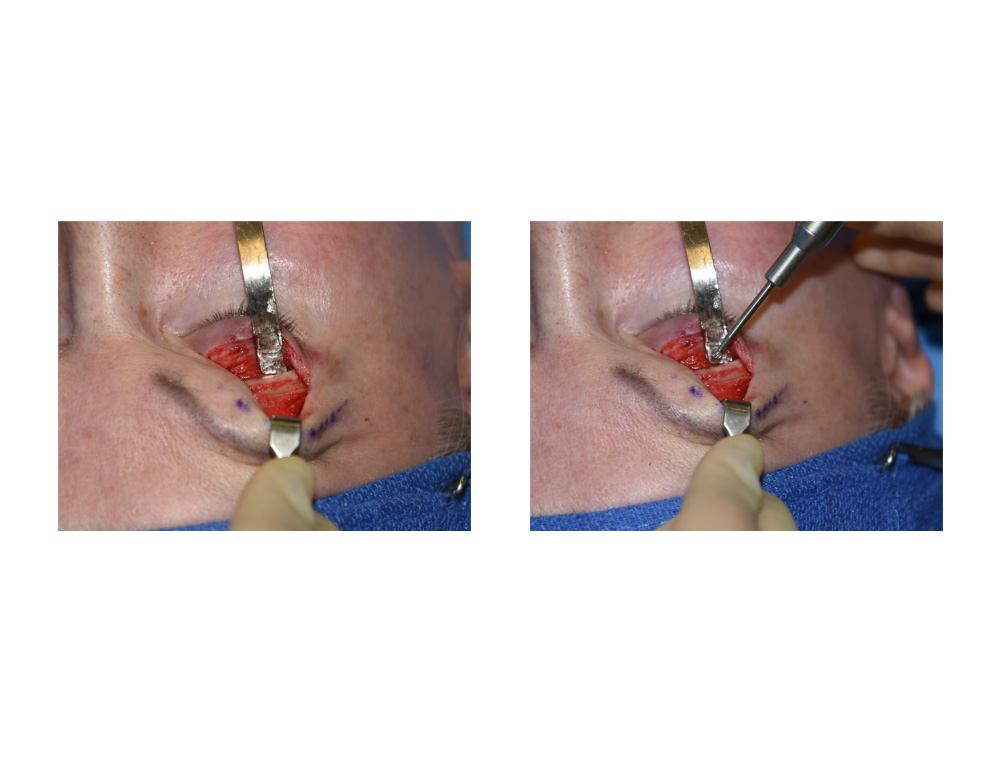 Transpalpebral brow bone reduction is limited in that it can not reach the more medial part of the brow bone due to the location of the supraorbital nerves. But for tail of the brow bone reshaping or pure vertical reduction of the supraorbital rim, an eyelid incision is more appealing than the ‘far away’ and more extensive coronal incisional approach.
Transpalpebral brow bone reduction is limited in that it can not reach the more medial part of the brow bone due to the location of the supraorbital nerves. But for tail of the brow bone reshaping or pure vertical reduction of the supraorbital rim, an eyelid incision is more appealing than the ‘far away’ and more extensive coronal incisional approach.
Dr. Barry Eppley
Indianapolis, Indiana