

There are numerous aesthetic chin surgeries which largely differ by the dimensions that are being changed. Chin reduction, just like chin augmentation, can be done in all three dimensions. (decreased horizontal projection, decreased height and decreased width) Such chin reductions are usually multidimensional (e.g., decreased projection and less height) and some even combine a reduction and an augmentation change. (e.g., less width and more projection)
Probably the least common reductive chin change is vertical or height reduction. This is for the long chin which has good projection and adequate width. This is typically viewed as a long lower third of the face and is often done to balance out the proportions of the facial thirds. (facial shortening)
While pure vertical chin reduction can be done from a submental approach by excision of the lower end of the chin bone, it is probably preferred in most cases to do it by an intraoral approach. With the intraoral approach a wedge of vertical chin bone is still removed. But instead of at the bottom of the chin bone by ostectomy, which requires complete degloving of the attached soft tissues, it is done by osteotomy in the middle of the chin bone. (interpositional removal) This has the advantage of keeping the soft tissues attached to the lower edge of the chin bone where they move upward with it as the bone is put back together.

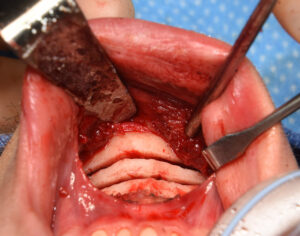
 Vertical chin reduction by osteotomy is done from an intraoral approach. An 8 to 10mm height of bone to be removed in marked in the midline well below the roots of the lower teeth. A initial low horizontal bone cut is made by a reciprocating saw in a near complete bicortical fashion.
Vertical chin reduction by osteotomy is done from an intraoral approach. An 8 to 10mm height of bone to be removed in marked in the midline well below the roots of the lower teeth. A initial low horizontal bone cut is made by a reciprocating saw in a near complete bicortical fashion.
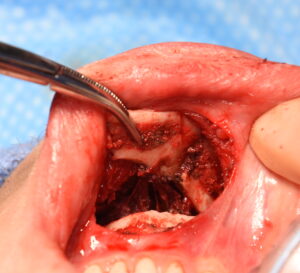 Then a second bone cut is made above it which tapers outward to meet the lower bone cut at the inferior border. Then both bone cuts are completed and the intervening wedge of bone removed. In removing this bone there will be attachments of the genioglossus muscle which will need to be released.
Then a second bone cut is made above it which tapers outward to meet the lower bone cut at the inferior border. Then both bone cuts are completed and the intervening wedge of bone removed. In removing this bone there will be attachments of the genioglossus muscle which will need to be released.
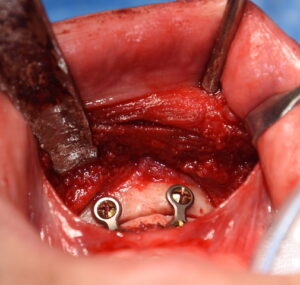
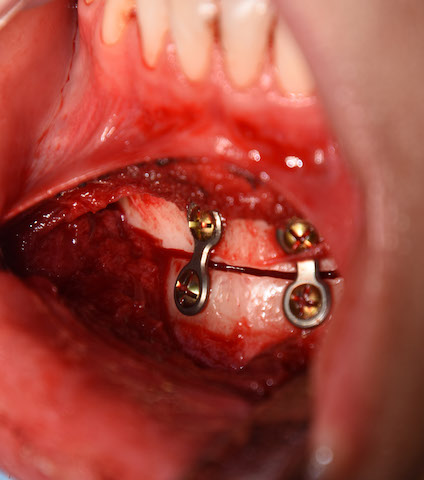
 The down fractured chin bone is then brought and put back together to the upper chin bone with small two-two-hole plates and screws. The chin is then vertically shortened by the amount of intervening bone removed.
The down fractured chin bone is then brought and put back together to the upper chin bone with small two-two-hole plates and screws. The chin is then vertically shortened by the amount of intervening bone removed.
While very effective it is important to point out that anterior chin shortening will disrupt the smooth inferior border line of the lower jaw from the jaw angles to the chin. As the chin is shortened the anterior line of the lower jaw is turned a bit upwards. This is mainly reflected in being able to feel a bump where the lateral osteotomy line ends. Healing will soften this bony bump but it will always be there to some degree.
Dr. Barry Eppley
Indianapolis, Indiana