

The webbed neck occurs is a wide variety of medical conditions and has variable presentations. While most commonly associated with Turner’s, Noonan and Klippel-Feil syndromes where the webbed necks are severe, they also occur in lesser presentations that may have no specific syndrome associated with them. While non-syndromic neck webbing is less severe, it may be more aesthetically disturbing given that it is a solitary physical deformity.
 The traditional methods of webbed neck correction use incisions and tissue rearrangements directly along the neck webs which are aesthetically unacceptable. While effective the visible scarring is not a worthy tradeoff in many cases particularly in the less severe neck webs. For this reason I use a posterior approach that employs a diamond-shaped skin excision. The upper half is in the hairline and the lower half is in the non-hair bearing neck skin. The middle angles of the equilateral parallelogram are placed along the horizontal axis of the maximum amount of inward skin pull needed.
The traditional methods of webbed neck correction use incisions and tissue rearrangements directly along the neck webs which are aesthetically unacceptable. While effective the visible scarring is not a worthy tradeoff in many cases particularly in the less severe neck webs. For this reason I use a posterior approach that employs a diamond-shaped skin excision. The upper half is in the hairline and the lower half is in the non-hair bearing neck skin. The middle angles of the equilateral parallelogram are placed along the horizontal axis of the maximum amount of inward skin pull needed.
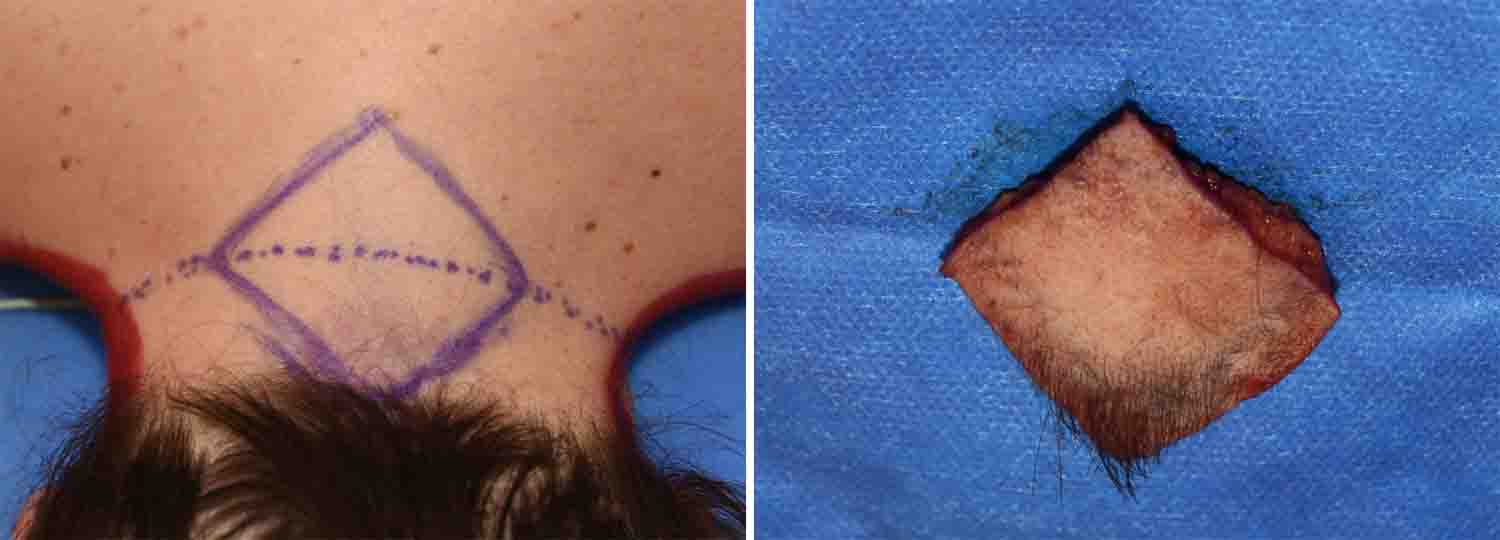
 The posterior neck skin is fully excised down to the fascia. It can be surprising how thick the skin and fat is on the back of the neck even in a thin person. Skin flaps are raised out to the lateral neck web lines on each side along the trapezius fascia. The fascia is opened along a linear line that goes out to the neck webs. With the trapezius muscle exposed its fibers are partially released from its lateral border for several centimeters inward. Midline fascial plication is then done on each side pulling in the sides of the muscle.
The posterior neck skin is fully excised down to the fascia. It can be surprising how thick the skin and fat is on the back of the neck even in a thin person. Skin flaps are raised out to the lateral neck web lines on each side along the trapezius fascia. The fascia is opened along a linear line that goes out to the neck webs. With the trapezius muscle exposed its fibers are partially released from its lateral border for several centimeters inward. Midline fascial plication is then done on each side pulling in the sides of the muscle.
 To complete the webbed neck correction, the skin is closed by changing the diamond-shaped excision into a vertical midline closure. The muscle and fascia work brings in the deeper structures while the skin closure provides the more superficial neck narrowing effect. Skin excision and closure alone will not create a sustained webbed neck corection.
To complete the webbed neck correction, the skin is closed by changing the diamond-shaped excision into a vertical midline closure. The muscle and fascia work brings in the deeper structures while the skin closure provides the more superficial neck narrowing effect. Skin excision and closure alone will not create a sustained webbed neck corection.
Dr. Barry Eppley
Indianapolis, Indiana