

The endoscopic brow lift has been the most popular forehead rejuvenation technique for some time now. Its appeal is that it eliminates most of the scalp or hairline scarring that occurs from either the traditional coronal or pretrichial incisional approaches. While this is certainly true it is also important to remember that it is not effective or indicated for all types of brow ptosis or sagging. Patients with very deep forehead and glabellar rhytids or a long skin distance between the eyebrows and the frontal hairline may be better served by these more long incision brow lift approaches.
 The endoscopic brow lift is predicated on three basic principles, limited small separate scalp incisions for endoscopic access and instrument dissection, a deep subperiosteal brow bone tissue release and bone fixation of the elevated forehead/brow tissues. Such scalp incisions are usually four with the more central paramedic ones centered over the vertical direction of the desired inner brow pull.
The endoscopic brow lift is predicated on three basic principles, limited small separate scalp incisions for endoscopic access and instrument dissection, a deep subperiosteal brow bone tissue release and bone fixation of the elevated forehead/brow tissues. Such scalp incisions are usually four with the more central paramedic ones centered over the vertical direction of the desired inner brow pull.
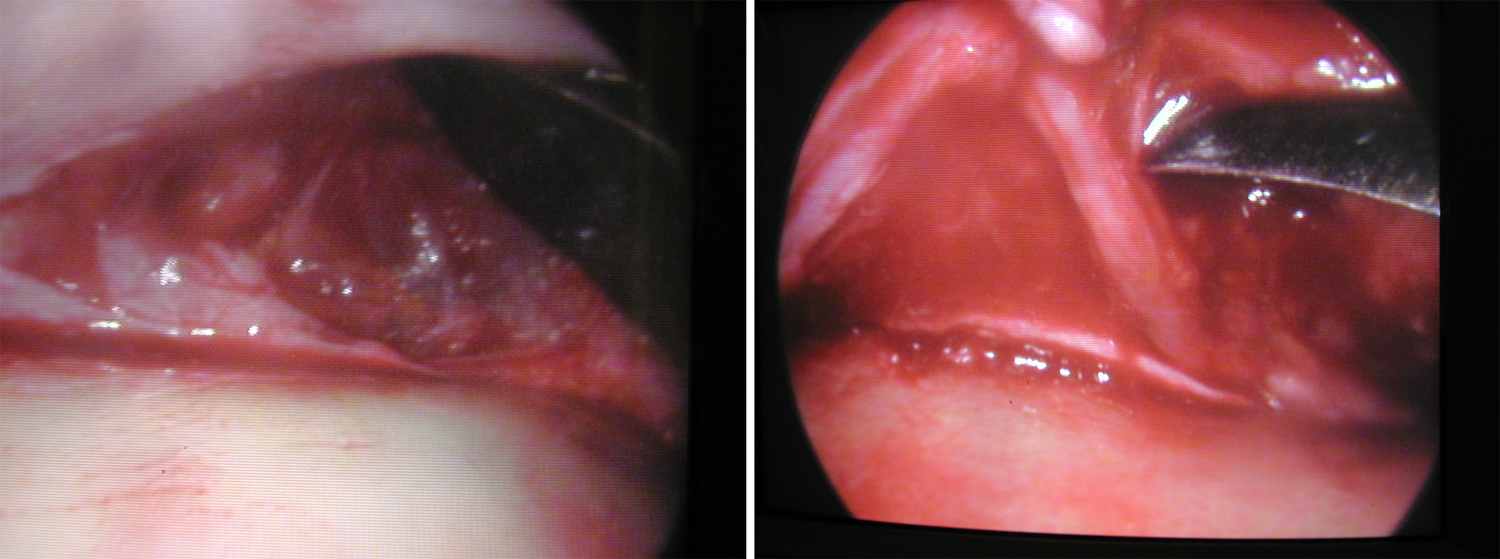 The endoscope allows the periorbital tissues to elevated off of the forehead and down to the brow bones. At this point the periosteum is opened and the supraorbital nerves dissected out with glabellar muscle release around them. The periosteal release must be carried out along the entire brow bone edges from one lateral orbit to the other.
The endoscope allows the periorbital tissues to elevated off of the forehead and down to the brow bones. At this point the periosteum is opened and the supraorbital nerves dissected out with glabellar muscle release around them. The periosteal release must be carried out along the entire brow bone edges from one lateral orbit to the other.
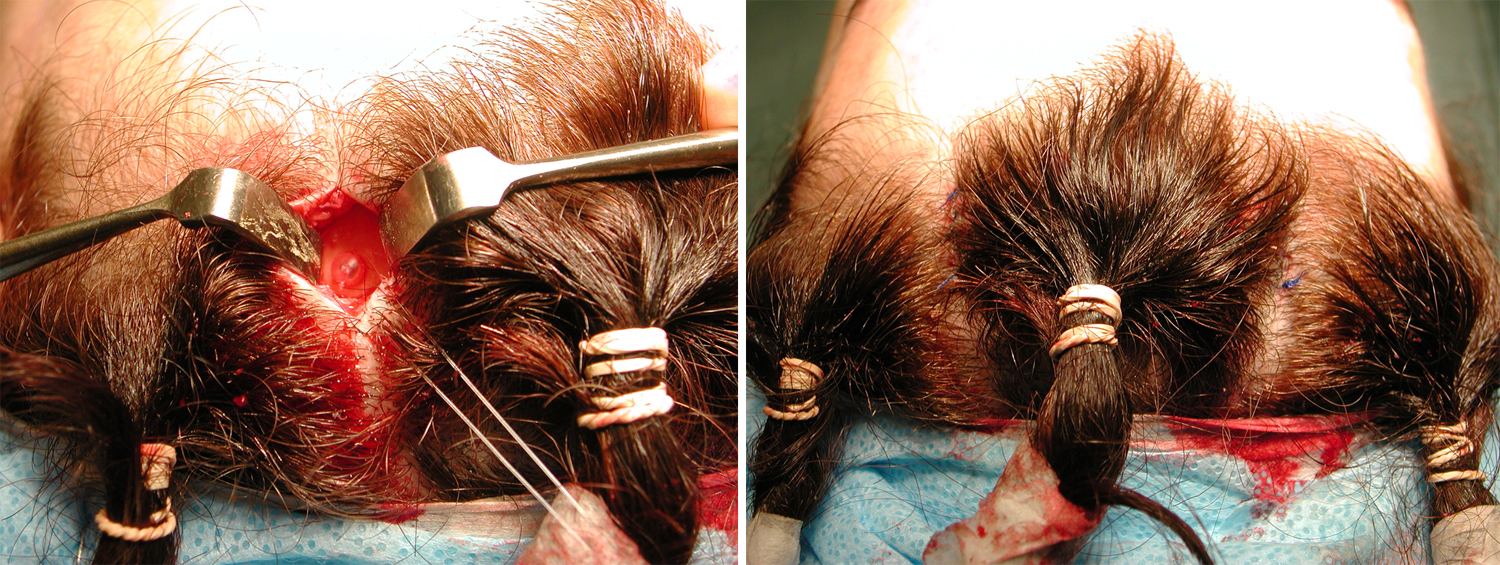
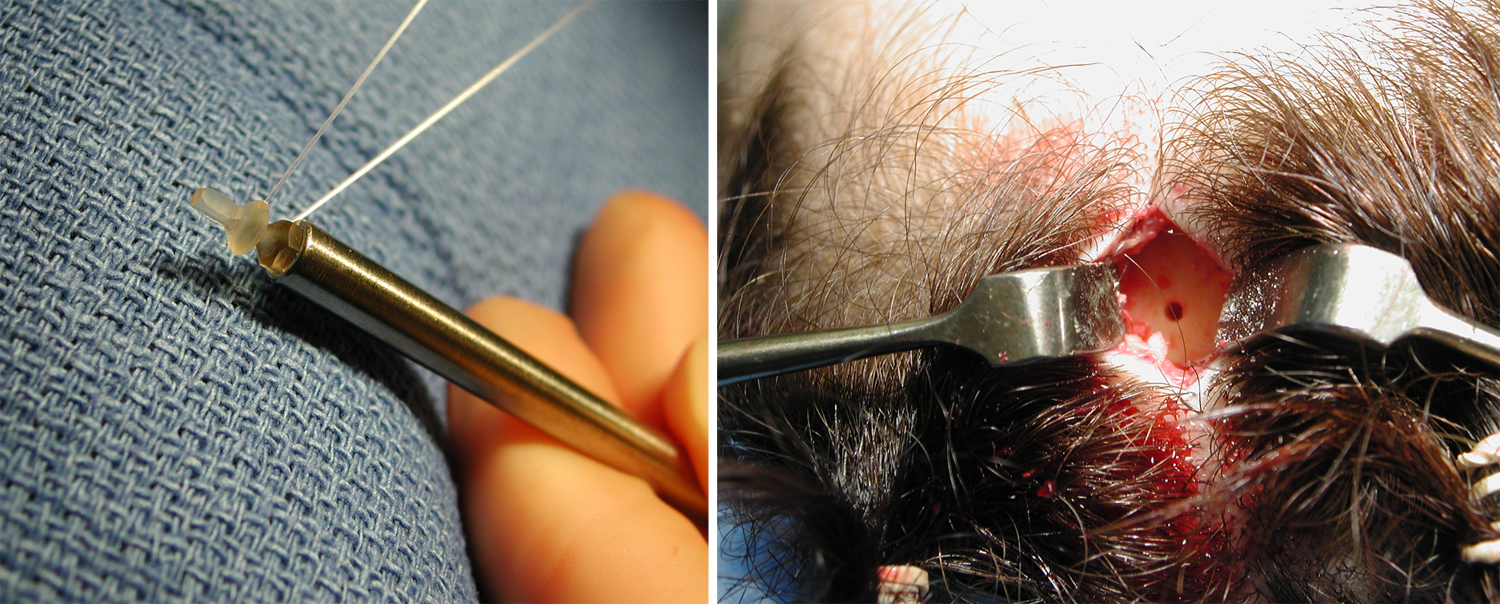 One of the key elements of the success of the endoscopic brow lift is the fixation of the elevated brow tissues. Many techniques have been described for it but my favorite continues to be suture anchorage to the bone using a screw. The screw I prefer is the Lactosorb endobrow screw. It has a hole in the top of the screw through which a suture can be passed, making it in effect an intraoperatively fashioned suture anchor. A hole is made in the bone by a handpieee and burr into the resorbable screw is pushed and locked into place. The needle of the suture is then used to to grasp the galea of the elevated forehead flap and tied down.
One of the key elements of the success of the endoscopic brow lift is the fixation of the elevated brow tissues. Many techniques have been described for it but my favorite continues to be suture anchorage to the bone using a screw. The screw I prefer is the Lactosorb endobrow screw. It has a hole in the top of the screw through which a suture can be passed, making it in effect an intraoperatively fashioned suture anchor. A hole is made in the bone by a handpieee and burr into the resorbable screw is pushed and locked into place. The needle of the suture is then used to to grasp the galea of the elevated forehead flap and tied down.
 While the head of the polymer endoscrew may be felt for several months after surgery, it will disappear through a natural hydrolytic resorption process. This is long after the forehead flap has healed back down to the skull bone in its elevated position.
While the head of the polymer endoscrew may be felt for several months after surgery, it will disappear through a natural hydrolytic resorption process. This is long after the forehead flap has healed back down to the skull bone in its elevated position.
Dr. Barry Eppley
Indianapolis, Indiana