

Buttock augmentation by injection fat grafting, known by the urban term of Brazilian Butt Lift or BBL, has been the fastest growing body contouring procedure in the past decade. Because it is ‘fat recycling’ procedure offers the dual benefit of reduction of undesired body contours by the liposuction harvest and the increase in buttock size by its relocation to this body area.
But despite its popularity and wide spread use, it has proven to also be a procedure that is not without its risks. Recent studies have shown that there are more major complications from this procedure than is commonly known with the highest mortality rate of any modern day cosmetic surgery procedure. Such events are related to pulmonary fat emboli in most cases. At roughly a death in every 3500 procedures done this is unacceptable in cosmetic surgery.
In the January 2018 issue of the journal Plastic and Reconstructive Surgery an article was published entitled ‘Staying Safe During Gluteal Fat Transplantation’. In this paper the authors review the important techniques of more safely performing fat injections to the buttocks based on patient selection, instrumentation, patient positioning and injection techniques based on buttock anatomy and vasculature. This is fundamentally about avoiding injuring deep gluteal vessels and inadvertently getting the fat transfer into them.
The anatomy of the buttocks is divided into superficial and deep levels. The superficial level consists of the gluteus maximus, gluteus minimus and tensor fascia late muscles. The deep muscles are smaller and include the piriformis, gemellus superior and inferior and quadratus femoris. The inferior and superior gluteal vessels originate from below the prirformis but emerge out onto the outer surfaces of the gemellus and piriformis. Most relevantly are these deeper gluteal veins which are surprisingly big (5 to 6m) and are felt to be the most common entrance for fat emboli from fat injections.
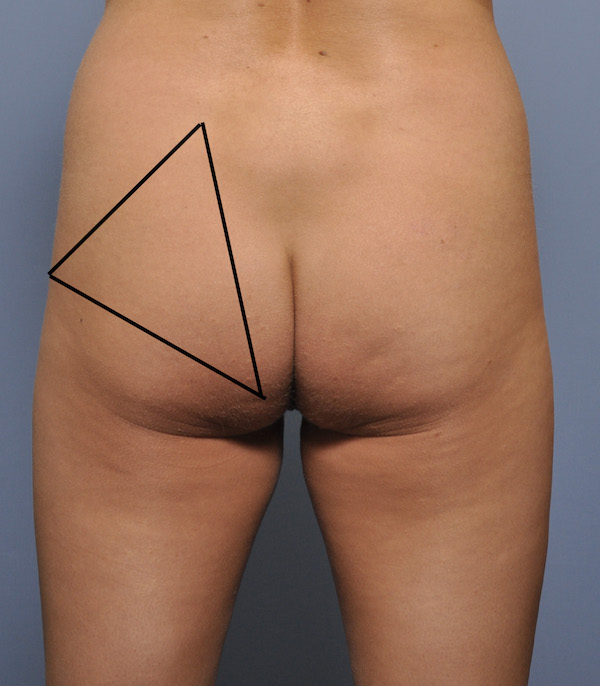 The danger one in buttock augmentation is a triangle between the posterior superior iliac spine superiorly, the greater trochanter laterally and the inferior ischial tuberosity. Deep fat injections should be avoided in this area in particular as that is where the deep gluteal vessels lie.
The danger one in buttock augmentation is a triangle between the posterior superior iliac spine superiorly, the greater trochanter laterally and the inferior ischial tuberosity. Deep fat injections should be avoided in this area in particular as that is where the deep gluteal vessels lie.
Preoperative patient selection should be on avoiding patients that have a history of deep vein thrombosis, pulmonary emboli, large varicose veins or sciatic nerve symptoms.
Fat injection buttock augmentation is done in the prone position with the hips flexed. (jack knife position) In this position the knees should be bent to avoid venous polling in the calfs. This position also allows for more certainty that the fat is injected into the subcutaneous and superficial muscles.
 The injected fat should be done using larger cannulas. (blunt tipped and greater than 4mm in diameter) This cannula size combined with a continuous back and forth cannular motion significantly decreases the risk of venous injury and fat introduction. The buttocks should also not be filled to the point of high internal pressure where the fat comes squirting back out from the skin entrance site. By my own personal experience i would also only inject from a superior direction which, in the jackknife position, ensures a superficial injection plane and no change to get under the gluteus maximus muscle.
The injected fat should be done using larger cannulas. (blunt tipped and greater than 4mm in diameter) This cannula size combined with a continuous back and forth cannular motion significantly decreases the risk of venous injury and fat introduction. The buttocks should also not be filled to the point of high internal pressure where the fat comes squirting back out from the skin entrance site. By my own personal experience i would also only inject from a superior direction which, in the jackknife position, ensures a superficial injection plane and no change to get under the gluteus maximus muscle.
Dr. Barry Eppley
Indianapolis, Indiana