


 One of the most popular uses of the custom facial implant concept is that of the jawline. The combination of no off-the-shelf implant that can accomplish a total jaw augmentation result and its powerful effect on the appearance of the lower third of the face the custom jawline implant is a facial game changer for many facial reshaping patients.
One of the most popular uses of the custom facial implant concept is that of the jawline. The combination of no off-the-shelf implant that can accomplish a total jaw augmentation result and its powerful effect on the appearance of the lower third of the face the custom jawline implant is a facial game changer for many facial reshaping patients.
But just because it is custom designed on the patient’s own 3D CT scan is not an assurance that the patient’s aesthetic jaw augmentation goals will be precisely achieved. The reality of custom facial implants is that 30% to 40% of such patients will desire to undergo a revision to improve their aesthetic outcomes. This is a reflection of the fact that currently there is no method to know before surgery what the exact effects of the chosen implant dimensions will do. The most assured outcomes are when patients have indwelling implants whose aesthetic effects are known and then it is more predictable to design around them.
 The custom jawline implant in my experience has the greatest potential for revision of all the custom facial implants. This is because of the large bony surface area that it covers and having three major points of projection with different shapes. (chin and jaw angles) The reasons for revisions can be because it’s effects are too strong, not strong enough or the desire for an improved shape of some part of it
The custom jawline implant in my experience has the greatest potential for revision of all the custom facial implants. This is because of the large bony surface area that it covers and having three major points of projection with different shapes. (chin and jaw angles) The reasons for revisions can be because it’s effects are too strong, not strong enough or the desire for an improved shape of some part of it

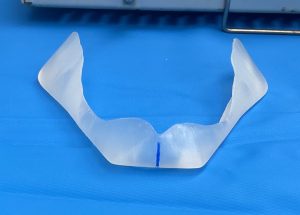
The most common design error in hindsight is in making the implant or some part of it too big. Fortunately this is the ‘easiest’ implant dimension to change. (easy as defined by not having to make a new implant) Such intraoperative modifications can be done by shaving the implant down using large blade scalpels. Such implant sculpting is a learned skill but becomes necessary if one does many custom facial implants. Too much jaw angle flare/thickness or a chin that is too wide are the most common culprits.
The custom jawline implant is ultimately ‘customizable’ whether by a recognized need for a dimensional change during its initial placement or on a secondary basis. Long controlled strokes with a #10 or #20 scalpel blade enables a well shaped reduction.
Dr. Barry Eppley
Indianapolis, Indiana