

 The use of injectable fillers in the treatment of temporal hollowing is common. It can be debated whether the hollowing is due to fat atrophy, muscle thinning or both. Contemporary thought is that temporal hollowing is due to fat atrophy, hence the targeting of injectable filler placement into the temporal fat pad regions. It is also important to recognize that temporal hollowing in many young patients is congenital and is the result of natural anatomy without any age-related changes.
The use of injectable fillers in the treatment of temporal hollowing is common. It can be debated whether the hollowing is due to fat atrophy, muscle thinning or both. Contemporary thought is that temporal hollowing is due to fat atrophy, hence the targeting of injectable filler placement into the temporal fat pad regions. It is also important to recognize that temporal hollowing in many young patients is congenital and is the result of natural anatomy without any age-related changes.
In the December 2021 issue of the Aesthetic Surgery Journal an article on published on this area of facial augmentation entitled ‘A New Target for Temple Volumization? An Anatomical and Ultrasound-Guided Study of the Intermediate Temporal Fat Pad’. In this paper the author performed an anatomical evaluation of an intermediate level of temporal augmentation. Specifically the anatomy of the intermediate temporal fat pad was examined by both ultrasound and dye injections in twenty fresh cadavers. Cross-sectional dissection was done to evaluate injection accuracy. A single clinical case was done with ultrasound-guided injected saline.
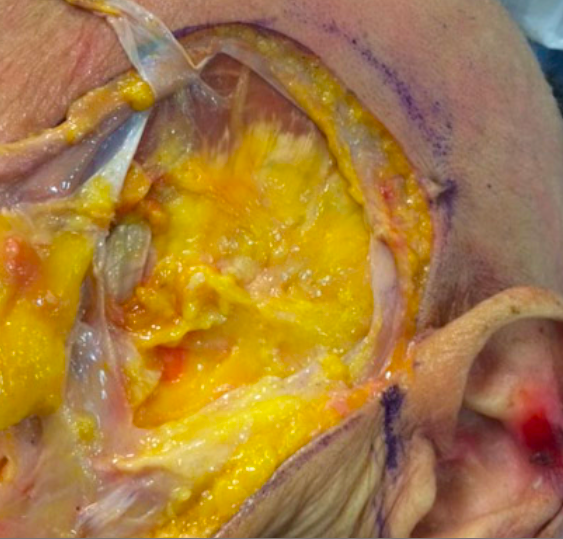
 In 90% of the cadaveric injections the dye was properly placed into the intermediate temporal fat pad. The other 10% of the dye injections ended up beneath the deep temporal fascia into the temporal muscle. In the one clinical case saline was successfully injected into the fat pad. Anatomically the intermediate fat pad is located in the most anterior and inferior temporal region. This places it at the junction of the lateral orbital rim and the zygomatic arch…which is also the deepest part of the temporal area in terms of thickness of the temporal muscle and distance between the skin and the underlying bony temporal fossa. It sits just above the deep temporal fascia and thus is a suprafascial injection site.
In 90% of the cadaveric injections the dye was properly placed into the intermediate temporal fat pad. The other 10% of the dye injections ended up beneath the deep temporal fascia into the temporal muscle. In the one clinical case saline was successfully injected into the fat pad. Anatomically the intermediate fat pad is located in the most anterior and inferior temporal region. This places it at the junction of the lateral orbital rim and the zygomatic arch…which is also the deepest part of the temporal area in terms of thickness of the temporal muscle and distance between the skin and the underlying bony temporal fossa. It sits just above the deep temporal fascia and thus is a suprafascial injection site.
While the intermediate temporal fat pad region can be accurately injected for aesthetic voluminization purposes, it is not clear whether doing so has any advantages over blind injection techniques. The most important location is to be certain the injectate sits above the deep temporal fascia where it can exert its greatest effects. The softness of filler materials does not provide a great push on the tight deep temporal fascia if placed below it. Implants do much better in the subfascial location where their increased stiffness and volume (even a thin temporal implant creates over 3ccs of a volume effect) provides a greater and permanent aesthetic effect.
Dr. Barry Eppley
Indianapolis, Indiana