

Rib removal is an operation that is done to improve the shape of the waistline. Specifically it is done to make the waistline more narrow which is associated with a more feminine appearance and can enhance the appearance of the breasts and hips above and below it. The traditional approaches for waistline reduction are liposuction and tummy tuck surgery which, while effective for many patients, works best when excesses of skin and fat are the major impediments to a smaller waistline. But for patients in which these are not major contributing factors or have already been treated, rib removal remains the only possible treatment option to consider.
The concept of rib removal surgery is based on removing the bony internal support at the waistline level, thus allowing the overlying soft tissues to collapse inward. The position and flare of the lower ribs does make a contribution to the waistline shape as can be easily felt with one’s own hands. But my approach to rib removal is more comprehensive. The tissues between the skin and the ribs can also be reduced at the same time.
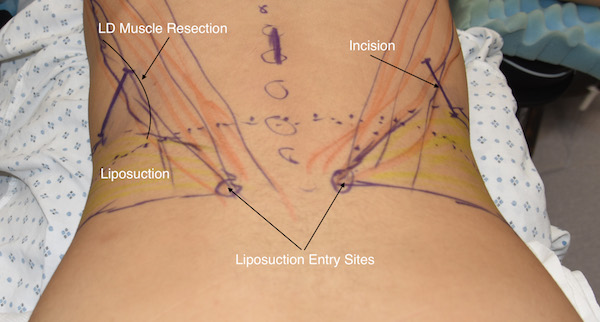
 Flank liposuction is an important component of rib removal surgery. Since the surgery is done in the prone position this is an ideal opportunity to treat flank fullness. Even in patients that have had prior flank liposuction or BBL surgery some additional fat aspirate can always be obtained. The entrance sites for the cannula are the dimples of Venus location bilaterally. These will also serve as the exit sites for drains from the rib removal sites.
Flank liposuction is an important component of rib removal surgery. Since the surgery is done in the prone position this is an ideal opportunity to treat flank fullness. Even in patients that have had prior flank liposuction or BBL surgery some additional fat aspirate can always be obtained. The entrance sites for the cannula are the dimples of Venus location bilaterally. These will also serve as the exit sites for drains from the rib removal sites.
 The location of the small 5cm long back incisions for rib removal is critical. They must be placed directly over rib #11 and just at the lateral border of the latissimus dorsi muscle. Since the size of the incision limits the ability to go too far north or south of it, removing rib segments from #10, #11 and #12 requires precise incision placement. One can only go one rib above and below it. This incision location is always higher and more to the side of the back than one would initially think.
The location of the small 5cm long back incisions for rib removal is critical. They must be placed directly over rib #11 and just at the lateral border of the latissimus dorsi muscle. Since the size of the incision limits the ability to go too far north or south of it, removing rib segments from #10, #11 and #12 requires precise incision placement. One can only go one rib above and below it. This incision location is always higher and more to the side of the back than one would initially think.
 Despite that the skin can act like a ‘mobile window’, the rib lengths removed are longer than the skin incision particularly ribs #10 and #11. Thus a tunnel technique must be used to maximize the rib removals. This is done by cutting the rib at a proximal location first and then pulling it up through the incision as it is dissected out distally to its cartilaginous end. Once the rib is cut it is dissected circumferentially as it pulled up through the incision. This leaves a perichondrial tunnel behind into which Exparel-soaked gelfoam sponges can be be placed to help with postoperative discomfort management.
Despite that the skin can act like a ‘mobile window’, the rib lengths removed are longer than the skin incision particularly ribs #10 and #11. Thus a tunnel technique must be used to maximize the rib removals. This is done by cutting the rib at a proximal location first and then pulling it up through the incision as it is dissected out distally to its cartilaginous end. Once the rib is cut it is dissected circumferentially as it pulled up through the incision. This leaves a perichondrial tunnel behind into which Exparel-soaked gelfoam sponges can be be placed to help with postoperative discomfort management.
 The lengths of the ribs that need to be removed is often misunderstood. The entire rib length is not what is taken. Only a portion of the outer half of the rib needs to be removed. Any portion of the rib that lies inside the lateral border of the erector spine muscle does not contribute to waistline support. Of the three ribs removed, the longest lengths comes from #10 and #11. While the end of rib #12 is always removed it contributes the least to waistline reduction.
The lengths of the ribs that need to be removed is often misunderstood. The entire rib length is not what is taken. Only a portion of the outer half of the rib needs to be removed. Any portion of the rib that lies inside the lateral border of the erector spine muscle does not contribute to waistline support. Of the three ribs removed, the longest lengths comes from #10 and #11. While the end of rib #12 is always removed it contributes the least to waistline reduction.
 One significant contributor to waistline width is the outer edge of the latissimus dorsi muscle. Being up to 20mms thick in some patients, its reduction can be helpful. It is necessary to pass through this muscle for rib access so removing several centimeters of its lateral width over the rib removal sites has a dual benefit both intra- and postoperatively.
One significant contributor to waistline width is the outer edge of the latissimus dorsi muscle. Being up to 20mms thick in some patients, its reduction can be helpful. It is necessary to pass through this muscle for rib access so removing several centimeters of its lateral width over the rib removal sites has a dual benefit both intra- and postoperatively.
The tern rib removal surgery indicates that bone removal is all that is done during the procedure. But I have developed a more comprehensive approach to this waistline reduction surgery that maximizes its effects. If a patient is willing to submit to this type of aesthetic procedure, then every effort should be done to ensure the best result possible.
Dr. Barry Eppley
Indianapolis, Indiana