

The reduction of almost any facial bone is a lot more challenging than augmenting it. Unlike augmentation which pushes out the overlying soft tissue, eliminating any concern about adverse soft tissue effects, facial bone reductions always runs the risk of soft tissue laxity/sagging. In addition, while facial bone augmentations are achieved by a smooth implant surface, facial bone reductions can rarely be accomplished by a smooth-surfaced reduction.

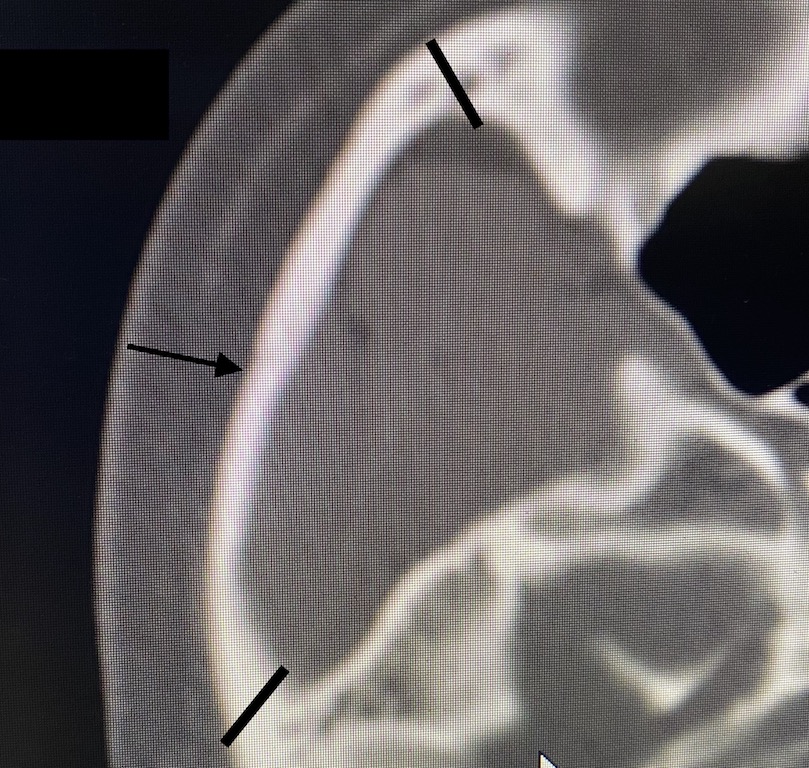
 In reducing wide cheekbones most of the excessive width is not located at the anterior end of the zygomatic body which can be accessed intraorally. Rather the width is located over the zygomatic arch due to its convexity. The more convex the zygomatic arch is the wider the cheek width is. The widest part of the cheek along the arch is the mid-arch suture line which represents the developmental merging of the face to the skull at the cheek level. It is typically the widest part of the cheek complex because the thick temporal muscle must pass underneath it. This does not have the same impact on width at the more anterior zygomatic body. (main cheekbone)
In reducing wide cheekbones most of the excessive width is not located at the anterior end of the zygomatic body which can be accessed intraorally. Rather the width is located over the zygomatic arch due to its convexity. The more convex the zygomatic arch is the wider the cheek width is. The widest part of the cheek along the arch is the mid-arch suture line which represents the developmental merging of the face to the skull at the cheek level. It is typically the widest part of the cheek complex because the thick temporal muscle must pass underneath it. This does not have the same impact on width at the more anterior zygomatic body. (main cheekbone)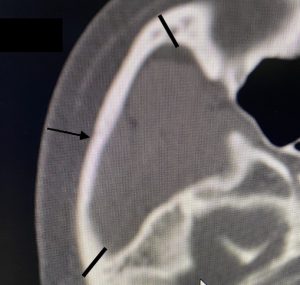
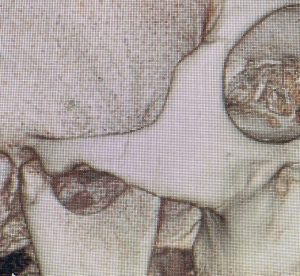
Thus to reduce cheekbone width it is about changing the outward position of the zygomatic arch. It is inaccessible for any attempt at burring reduction and, even if it weren’t, it is a very thin bone of a only a few millimeters thickness. In addition it is the origin of the masseter muscle and these attachments do not want to be lost. Osteotomies of its front and back attachments and moving in the whole arch inward is what is required for reducing wide cheekbones.
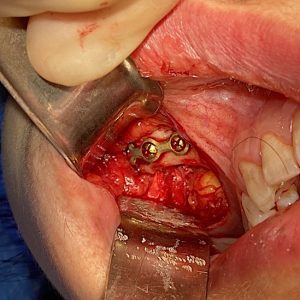 Performing these cheekbone (arch) osteotomies requires a dual incisional approach to access each end of the arch. The intraoral approach to the anterior end is the obvious one due to it being the same incision used for cheek augmentation. Various osteotomy patterns have been described for the anterior cheek bone cut. But regardless of the pattern of the bone cut, its inward relocation must be supported by plate and screw fixation. The downward pull of the masseter muscle can cause displacement of the bone and, at the least, can contribute to soft tissue cheek sagging.
Performing these cheekbone (arch) osteotomies requires a dual incisional approach to access each end of the arch. The intraoral approach to the anterior end is the obvious one due to it being the same incision used for cheek augmentation. Various osteotomy patterns have been described for the anterior cheek bone cut. But regardless of the pattern of the bone cut, its inward relocation must be supported by plate and screw fixation. The downward pull of the masseter muscle can cause displacement of the bone and, at the least, can contribute to soft tissue cheek sagging.

 The osteotomy of the posterior zygomatic arch, however, must be done from a different incisional approach. This requires a direct incision right over its posterior end. An external skin incision at the back end of the sideburn (male) or preauricular tuft of hair (female) is needed. While the frontal branch of the facial nerve is in close proximity, its pathway is right in front of it. For this reason only blunt dissection is done from the skin down to the bone. The most proximal end of the zygomatic arch is identified when circumferential dissection can be done around it. An osteotome is used ti cut through it at an angle. Depending upon how much inward movement is needed either a self-locking technique or a small plate and screw is used for fixation.
The osteotomy of the posterior zygomatic arch, however, must be done from a different incisional approach. This requires a direct incision right over its posterior end. An external skin incision at the back end of the sideburn (male) or preauricular tuft of hair (female) is needed. While the frontal branch of the facial nerve is in close proximity, its pathway is right in front of it. For this reason only blunt dissection is done from the skin down to the bone. The most proximal end of the zygomatic arch is identified when circumferential dissection can be done around it. An osteotome is used ti cut through it at an angle. Depending upon how much inward movement is needed either a self-locking technique or a small plate and screw is used for fixation.

 Cheek width reduction can be effectively achieved by a dual osteotomy technique of the zygomatic arch. Its effects are immediate and, surprisingly, the postoperative swelling is less significant than in most facial augmentations. There has never been any facia bruising in my experience. Potential postoperative issues are asymmetry and soft tissue cheek sagging.
Cheek width reduction can be effectively achieved by a dual osteotomy technique of the zygomatic arch. Its effects are immediate and, surprisingly, the postoperative swelling is less significant than in most facial augmentations. There has never been any facia bruising in my experience. Potential postoperative issues are asymmetry and soft tissue cheek sagging.
Dr. Barry Eppley
Indianapolis, Indiana