

There are numerous areas of the face in which implants are used to create an aesthetic enhancement. Each one of these facial areas has their challenges for successful surgical placement. But the most difficult of them all is that of the jaw angle region of the lower face. The unique anatomy of the back part of the lower jaw makes jaw angle implants have a high incidence of malpositioning and increased implant revision rates.
There are numerous reasons that jaw angle implants are so challenging to successfully place including a posterior intraoral access (limited visibility) and that their are two sides. (hard to get perfectly symmetric placement) But the main reason for implant malposition is a lack of understanding of the muscle anatomy over the bone.
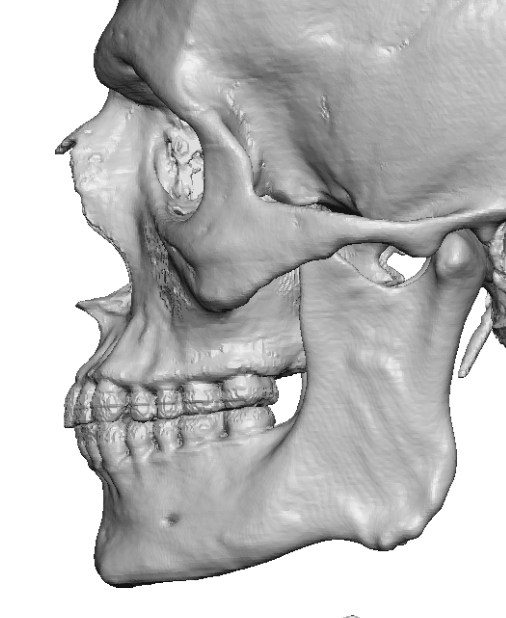
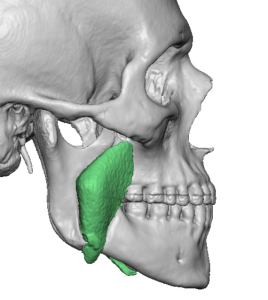
 The masseteric muscle has a broad origin along the zygomatic arch but it narrows down into a triangular shape as it approaches its insertion over the jaw angle bone. This narrowing of the muscle over the jaw angle allows for strong ligamentous attachments at the posterior and inferior jaw angle border as this is what the muscle pulls on to make the jaw move. If these ligamentous attachments are not elevated off of the bone, partially or completely, a jaw angle implant is not going to get into proper position. These ligamentous attachments are very visible…if you know to look for them. They are very obvious on 3D CT scans as bony bumps. Men have larger and more obvious ligamentous attachments than women. This is very different from the mentalis muscle of the chin where the insertion of the muscle is not on the lower chin bone but out onto the more superficial soft tissues.
The masseteric muscle has a broad origin along the zygomatic arch but it narrows down into a triangular shape as it approaches its insertion over the jaw angle bone. This narrowing of the muscle over the jaw angle allows for strong ligamentous attachments at the posterior and inferior jaw angle border as this is what the muscle pulls on to make the jaw move. If these ligamentous attachments are not elevated off of the bone, partially or completely, a jaw angle implant is not going to get into proper position. These ligamentous attachments are very visible…if you know to look for them. They are very obvious on 3D CT scans as bony bumps. Men have larger and more obvious ligamentous attachments than women. This is very different from the mentalis muscle of the chin where the insertion of the muscle is not on the lower chin bone but out onto the more superficial soft tissues.
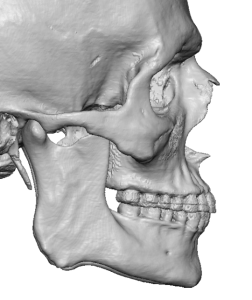
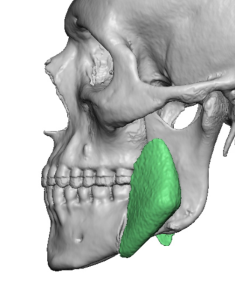
 Besides the ligamentous attachments it is important to realize that the jaw angles in most people are not in linear alignment with the jawline in front of it. They typically angle inward presumably to accommodate the size of the masseter muscle. Some surgeons may even confuse the ascending ramus at the anterior edge of the jaw angle as the posterior border. As a result some surgeons never dissect back far enough to reach the posterior border of the jaw angle, ending up having the implant being placed too far forward.
Besides the ligamentous attachments it is important to realize that the jaw angles in most people are not in linear alignment with the jawline in front of it. They typically angle inward presumably to accommodate the size of the masseter muscle. Some surgeons may even confuse the ascending ramus at the anterior edge of the jaw angle as the posterior border. As a result some surgeons never dissect back far enough to reach the posterior border of the jaw angle, ending up having the implant being placed too far forward.
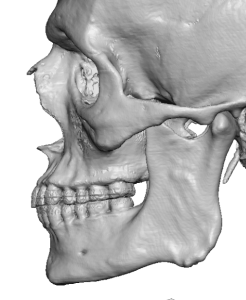
 Having seen many 3D CT scans with jaw angle implants on them it becomes easy to see classic patterns of jaw angle implant misplacements due to inadequate dissection. Some are so significant one wonders how they could have thought this was the correct implant placement. But they do illustrate what happens when the ligaments are not seen and/or released. And when the anterior bony landmarks of the jaw angle is confused with the posterior border.
Having seen many 3D CT scans with jaw angle implants on them it becomes easy to see classic patterns of jaw angle implant misplacements due to inadequate dissection. Some are so significant one wonders how they could have thought this was the correct implant placement. But they do illustrate what happens when the ligaments are not seen and/or released. And when the anterior bony landmarks of the jaw angle is confused with the posterior border.
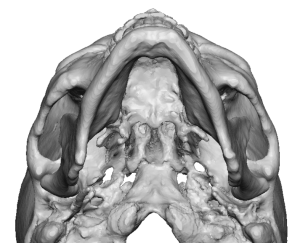
All surgical procedures of the jaw angles requires elevation of the bulk of the muscle in the bony recess above its posterior and inferior borders. Depending upon the procedure the insertion area directly over the angle may require elevation of varying degrees. But when an implant is being used to augment the jaw angles the ligamentous insertions always need to be lift off from the bone. This is particularly relevant when there is any amount of vertical lengthening required by the implant.
Dr. Barry Eppley
World-Renowned Plastic Surgeon