

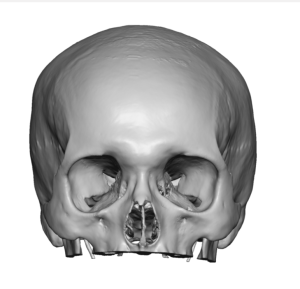
The wide head typically means an increased bitemporal distance which also gives it a more convex shape from the front view. While the bitemporal distance seems like a single area on the side of the head that is made of a uniformly thick temporal muscle, it is not that anatomically simple. The temporal area of the side of the head is large and extends from the side of the forehead all the way to the side of the occiput on the back of the head. But within this large surface area lies two different topographies of the muscle and bone that has great relevance to aesthetic head narrowing surgery.
In reducing the width of the side of the head it is muscle reduction that is required not bone. The thickness of the temporal muscle is influenced by the shape of the bone underneath it. While the temporal muscle is one contiguous muscle that does not have two different belies it does have two very different thicknesses. In reducing the muscle for decreasing head width the muscle is divided into an anterior and posterior areas based its two different thicknesses and in how it can be surgically treated.
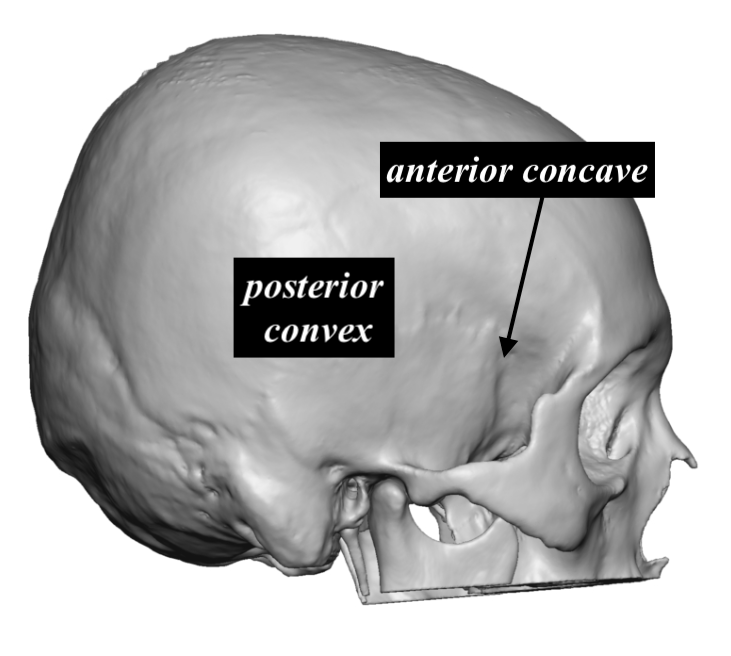
 The thickness of the temporal muscle is directly to the shape of the bone underneath it. The posterior temporal muscle is the thinnest section of the muscle due to the convex shape of the temporal bone underneath it. This is the section of the muscle that is completely removed in temporal reduction surgery which makes up 30% or less of the total temporal muscle mass. It is a highly effective procedure for reducing head width that is most evident above the ears. It is directly accessed by an incision behind the ear, making the procedure ‘scarless’.
The thickness of the temporal muscle is directly to the shape of the bone underneath it. The posterior temporal muscle is the thinnest section of the muscle due to the convex shape of the temporal bone underneath it. This is the section of the muscle that is completely removed in temporal reduction surgery which makes up 30% or less of the total temporal muscle mass. It is a highly effective procedure for reducing head width that is most evident above the ears. It is directly accessed by an incision behind the ear, making the procedure ‘scarless’.
 The anterior temporal region is very different. It has much thicker muscle due to the deep concave shape of the underlying bone. (temporal fossa) The size differential between it and the posterior region is at least 2X greater in thickness and often closer to 3X. It can not be directly accessed and its mass of muscle can not the completely removed. As a result a different surgical strategy is employed to reduce it. This entails a release at its origin long the bony temporal lone and transposition of the released muscle in a posterior superior direction. Unlike posterior temporal reduction no muscle is removed. (other than a small wedge near the incision to aid the transposition) The muscle is shifted and the final contour result depends on the combination of the immediate release and long term muscle atrophy from its decreased fiber length.
The anterior temporal region is very different. It has much thicker muscle due to the deep concave shape of the underlying bone. (temporal fossa) The size differential between it and the posterior region is at least 2X greater in thickness and often closer to 3X. It can not be directly accessed and its mass of muscle can not the completely removed. As a result a different surgical strategy is employed to reduce it. This entails a release at its origin long the bony temporal lone and transposition of the released muscle in a posterior superior direction. Unlike posterior temporal reduction no muscle is removed. (other than a small wedge near the incision to aid the transposition) The muscle is shifted and the final contour result depends on the combination of the immediate release and long term muscle atrophy from its decreased fiber length.
 When understanding the anatomy of the temporal muscle it is now easy to see that, while posterior temporal reduction can be done by itself, anterior temporal reduction requires a space to transpose the muscle. (posterior temporal muscle removal) Thus in total head widening reduction both anterior and posterior temporal reductions can be done from a single hidden incision.
When understanding the anatomy of the temporal muscle it is now easy to see that, while posterior temporal reduction can be done by itself, anterior temporal reduction requires a space to transpose the muscle. (posterior temporal muscle removal) Thus in total head widening reduction both anterior and posterior temporal reductions can be done from a single hidden incision.
Dr. Barry Eppley
World-Renowned Plastic Surgeon