

The sliding genioplasty is commonly performed chin reshaping surgery. While often perceived as a horizontal advancement procedure (and the autologous option for chin augmentation), it is far more dimensionally versatile. It can also provide vertical elongation or shortening as well as width reduction, all dimensional changes that an implant can not do.
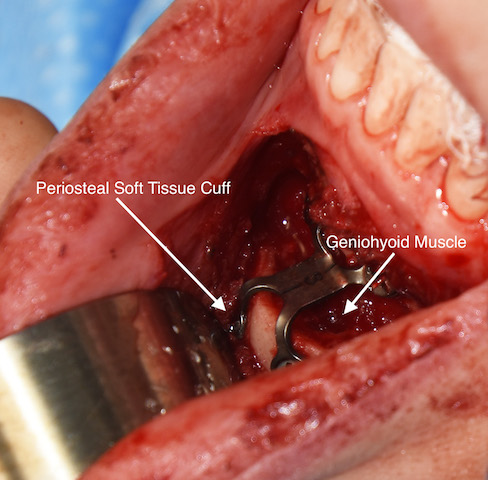
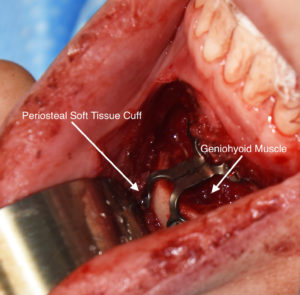 But despite the versatility of bony movements what is often not appreciated about the sliding genioplasty, and what makes it work (heal successfully), is an underappreciation of its blood supply. As the osteotomy line is completed and the inferior chin segment downfractured, the blood supply to the bone segment remains intact by perfusion through the inferior attached soft tissues. This is why, for example, the inferior chin segment can actually be advanced beyond bone contact with the superior segment and still survive and successfully heal. This is why the sliding genioplasty is anatomically known as a pedicled bone flap procedure.
But despite the versatility of bony movements what is often not appreciated about the sliding genioplasty, and what makes it work (heal successfully), is an underappreciation of its blood supply. As the osteotomy line is completed and the inferior chin segment downfractured, the blood supply to the bone segment remains intact by perfusion through the inferior attached soft tissues. This is why, for example, the inferior chin segment can actually be advanced beyond bone contact with the superior segment and still survive and successfully heal. This is why the sliding genioplasty is anatomically known as a pedicled bone flap procedure.
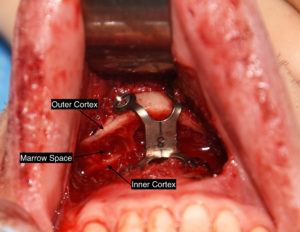
The visibility of the downfractured bleeding bone edges is a testament to its still robust blood supply after separation from the superior intact basal and alveolar bone segment. This is how every type facial osteotomy survives from the LeFort and Sagittal Split osteotomies…soft tissue attachments keep the cut mobilized bone segment alive.
Some patients are under the understandable but erroneous perception that the mobilized chin is a free floating bone segment. But without the perfusion supplied by its soft tissue attachments it would completely die and be resorbed. The maintenance of its blood supply also accounts for the incredibly low infection rate of the procedure. (I have only seen 2 infections in over 500 cases in the past 30 years)
Dr. Barry Eppley
Indianapolis, Indiana