

Cheek implant augmentation in a male must be considered differently than in a female. There are significant gender differences in the desired midface effect. Females typically desire a more anterior oval-shaped fullness that has been associated with attractive female faces. That is exactly the look that most men don’t want because it has a feminizing effect. Rather they prefer a higher augmentation that follows the natural skeletal line from just under the eye back along the zygomatic arch. This has a stronger skeletal look which is generally recognized with a more masculine face.
Some men that consider cheek implants also have an associated undereye deficiency or hollowing. This can be seen by a near or complete negative orbital vector which represents an infraorbital-malar skeletal deficiency. Because of the bony connections the flatter the cheek is the more recessed the infraorbital rim position becomes. This inward tilt to the superior support structures of the midface can not be properly addressed with any conventional cheek implant. Attempts to do often make the infraorbital rim deficiency more pronounced as this area is left untreated.
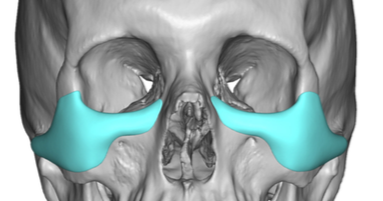
 The unique and larger surface area involvement of the undereye-cheek area requires a custom implant design approach to more completely treat it. Thus the concept of the custom infraorbital-malar implant. Besides the longer span of bone coverage the implant provides that turns the corner from the eye to the cheek in a connected fashion, this implant design provides a unique feature heretofore not seen….it can saddle the infraorbital rim. This raises the height of the bony infraorbital rim which has a better effect than any implant that merely provides horizontal augmentation in front of the rim. (effectively worsening undereye hollowing even if it fixes tear troughing) There are numerous points of dimensional thickness along the implant that need to be considered in the design but the impact of its horizontal bony area coverage accounts for its significant midfacial enhancement effect.
The unique and larger surface area involvement of the undereye-cheek area requires a custom implant design approach to more completely treat it. Thus the concept of the custom infraorbital-malar implant. Besides the longer span of bone coverage the implant provides that turns the corner from the eye to the cheek in a connected fashion, this implant design provides a unique feature heretofore not seen….it can saddle the infraorbital rim. This raises the height of the bony infraorbital rim which has a better effect than any implant that merely provides horizontal augmentation in front of the rim. (effectively worsening undereye hollowing even if it fixes tear troughing) There are numerous points of dimensional thickness along the implant that need to be considered in the design but the impact of its horizontal bony area coverage accounts for its significant midfacial enhancement effect.
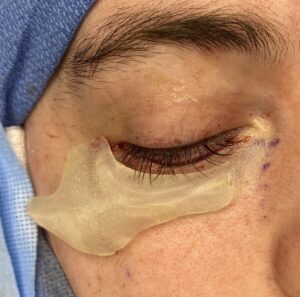


 Despite the length of the custom infraorbital-malar implant the transcutaneous lower eyelid approach is the best way to place it. It provides direct access and visualization for the critical place of the infraorbital part of the implant. This can be done using a partial lower eyelid incision with a very small lateral canthal extension. The intraoral approach creates a lot of stretch on the infraorbital nerve, which causes some duration of postoperative numbness, as well as increases the risk of infection. Its lack of superior visualization also makes placing the saddle portion of the implant on the rim less assured.
Despite the length of the custom infraorbital-malar implant the transcutaneous lower eyelid approach is the best way to place it. It provides direct access and visualization for the critical place of the infraorbital part of the implant. This can be done using a partial lower eyelid incision with a very small lateral canthal extension. The intraoral approach creates a lot of stretch on the infraorbital nerve, which causes some duration of postoperative numbness, as well as increases the risk of infection. Its lack of superior visualization also makes placing the saddle portion of the implant on the rim less assured.
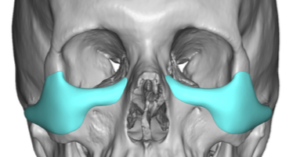
The high cheekbone look in a male requires a near or complete horizontal augmentation across the main body of the zygoma. Lack of cheek prominence is often associated with an infraorbital rim deficiency as well which is often seen as a negative orbital vector. The custom infraorbital-malar implant provides a complete bony augmentation across the middle line of the face which concurrently addresses undereye hollowing and lack of a defined cheek structure. It is somewhat similar to what is done in the lower face with a custom jawline implant where the entire horizontal line of the jaw is augmented.
Dr. Barry Eppley
Indianapolis, Indiana