

Of all the custom facial implants that are commonly used the infraorbital-malar (IOM) implant design is one of the most popular. It augments a skeletal unit of the face that is uniquely different from its separate parts of the cheek and infraorbital rim. As an implant that combines these two adjacent anatomic regions together it has the unique ability to treat a variety of midface aesthetic issues that are otherwise hard to find good solutions for historically. Deep undereye hollows, negative orbital vectors, narrow cheeks and achieving the high cheekbone looks are a few of the common uses for this implant design.
The IOM implant is very similar to that of an onlay over the entire ZMC bony region to create its effects. While the anterior projection to the infraorbital rim and lateral width to the entire zygoma is an obvious effect of such an implant design what is not as obvious is the ability to add vertical height to the infraorbital rim, extend upon along the lateral orbital wall or extend below the cheek onto the maxilla if desired.

 Because of its size the question is how is the custom IOM implant placed. While certain more modest designs can be introduced intraorally its long horizontal design favors a lower eyelid incisional approach for best placement.
Because of its size the question is how is the custom IOM implant placed. While certain more modest designs can be introduced intraorally its long horizontal design favors a lower eyelid incisional approach for best placement.
 But this lower eyelid incision is not a traditional lower blepharoplasty incision. Rather it is a more limited incision, a hemi-lid incision that starts with a 3mm lateral canthal incision and runs 1mm below the lashline inward to the pupillary level where it stops. A skin-muscle flap is raised and the entire subperiosteal pocket is developed from the nose medially to as far out onto the zygomatic arch as the implant design necessitates.
But this lower eyelid incision is not a traditional lower blepharoplasty incision. Rather it is a more limited incision, a hemi-lid incision that starts with a 3mm lateral canthal incision and runs 1mm below the lashline inward to the pupillary level where it stops. A skin-muscle flap is raised and the entire subperiosteal pocket is developed from the nose medially to as far out onto the zygomatic arch as the implant design necessitates.

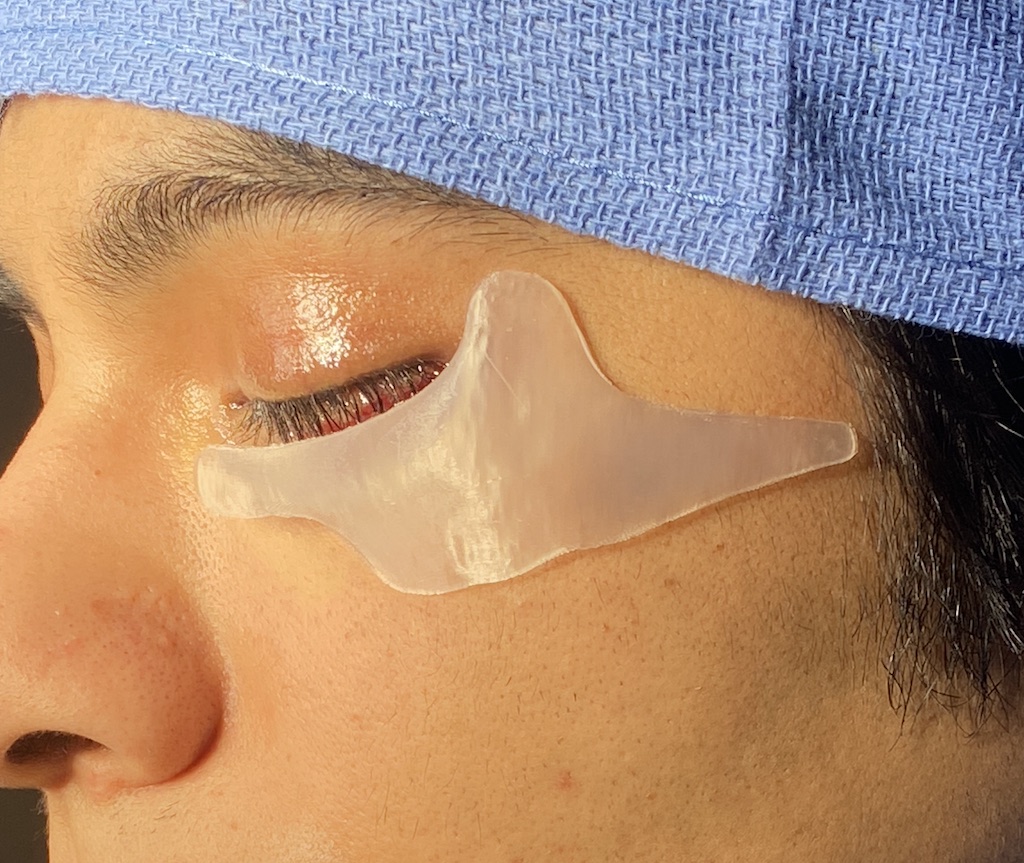
 Once the implant is inserted and positioned it is secured with a single titanium microscrew to the cheekbone. With a horizontally long implant it is critical to be sure the most medial infraorbital edge and the most lateral zygomatic arch edges of the implant are laying flat prior to placing the fixation.
Once the implant is inserted and positioned it is secured with a single titanium microscrew to the cheekbone. With a horizontally long implant it is critical to be sure the most medial infraorbital edge and the most lateral zygomatic arch edges of the implant are laying flat prior to placing the fixation.

 Closure is done in three layers with resorbable sutures with cheek suspension up tp the lateral orbital rim, orbicularis muscle reapproximation and skin closure.
Closure is done in three layers with resorbable sutures with cheek suspension up tp the lateral orbital rim, orbicularis muscle reapproximation and skin closure.

 The only dressing applied is taping of the lateral eyelid/cheek to help support it once the normal postoperative swelling sets in.
The only dressing applied is taping of the lateral eyelid/cheek to help support it once the normal postoperative swelling sets in.
The custom IOM implant despite its shape and size can be effectively placed through a lower eyelid incision with minimal scarring. This lower eyelid incision is different than the traditional lower blepharoplasty incision as it is performed in younger patients with better lid support and stronger tissue attachments. As no tissues are removed and it only crosses half of the lower eyelid less orbicularis muscle is disrupted. Collectively this translates into a much lower risk of any postoperative eyelid contraction deformities.
Dr. Barry Eppley
World-Renowned Plastic Surgeon