

Aesthetic augmentation of the midface has been traditionally done by off-the-shelf cheek implants. While different types of cheek implants exist they have their limitations based on the surface area of bone that they cover. Interestingly many styles of cheek implants are not designed to sit completely on the zygomatic major bone and to sit partially on the masseteric muscle fascia right beneath the bone. This is what creates the so called apple cheek effect which many females seek for their cheek augmentation.
But this lower anterior cheek augmentation effect is not typically what most men seek. They may desire that look if they have significant facial lipodystrophy and sunken in cheeks due to fat loss in more of a reconstructive approach. But from a pure aesthetic standpoint most men seek the classic high cheekbone look which historically has defied any exact method of doing so because no cheek implant has existed that create that effect. And when no standard implant exists to create a specific effect it is hard for surgeons to envision how to either create it or that even such an aesthetic facial need exists.
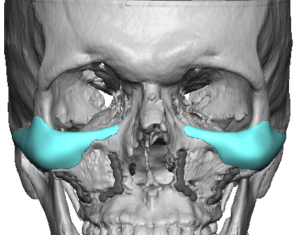

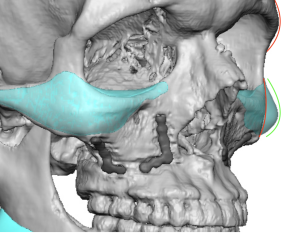
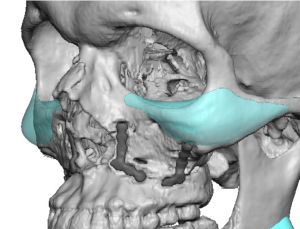
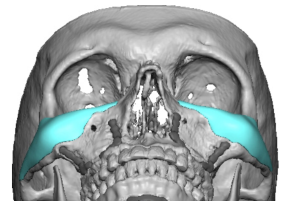 Custom implant designing change the whole paradigm on facial implant augmentations as virtually any implant design can be created that goes way beyond how any standard facial implant looks. This is well illustrated in one version of the high cheek bone look implant which otherwise is known as an infraorbital-malar (IOM) implant design. It provides an expansion of the skeletal contour along the horizontal bone line from the nasal bones out onto the zygomatic arch. While it can have an endless variety of shapes and dimensions along its course it is easy to see why it is called a high cheekbone implant style. Its value is that it converts a narrow ‘pinched’ midface and expands it outward, an effect that goes way beyond what a standard cheek implant can do.
Custom implant designing change the whole paradigm on facial implant augmentations as virtually any implant design can be created that goes way beyond how any standard facial implant looks. This is well illustrated in one version of the high cheek bone look implant which otherwise is known as an infraorbital-malar (IOM) implant design. It provides an expansion of the skeletal contour along the horizontal bone line from the nasal bones out onto the zygomatic arch. While it can have an endless variety of shapes and dimensions along its course it is easy to see why it is called a high cheekbone implant style. Its value is that it converts a narrow ‘pinched’ midface and expands it outward, an effect that goes way beyond what a standard cheek implant can do.
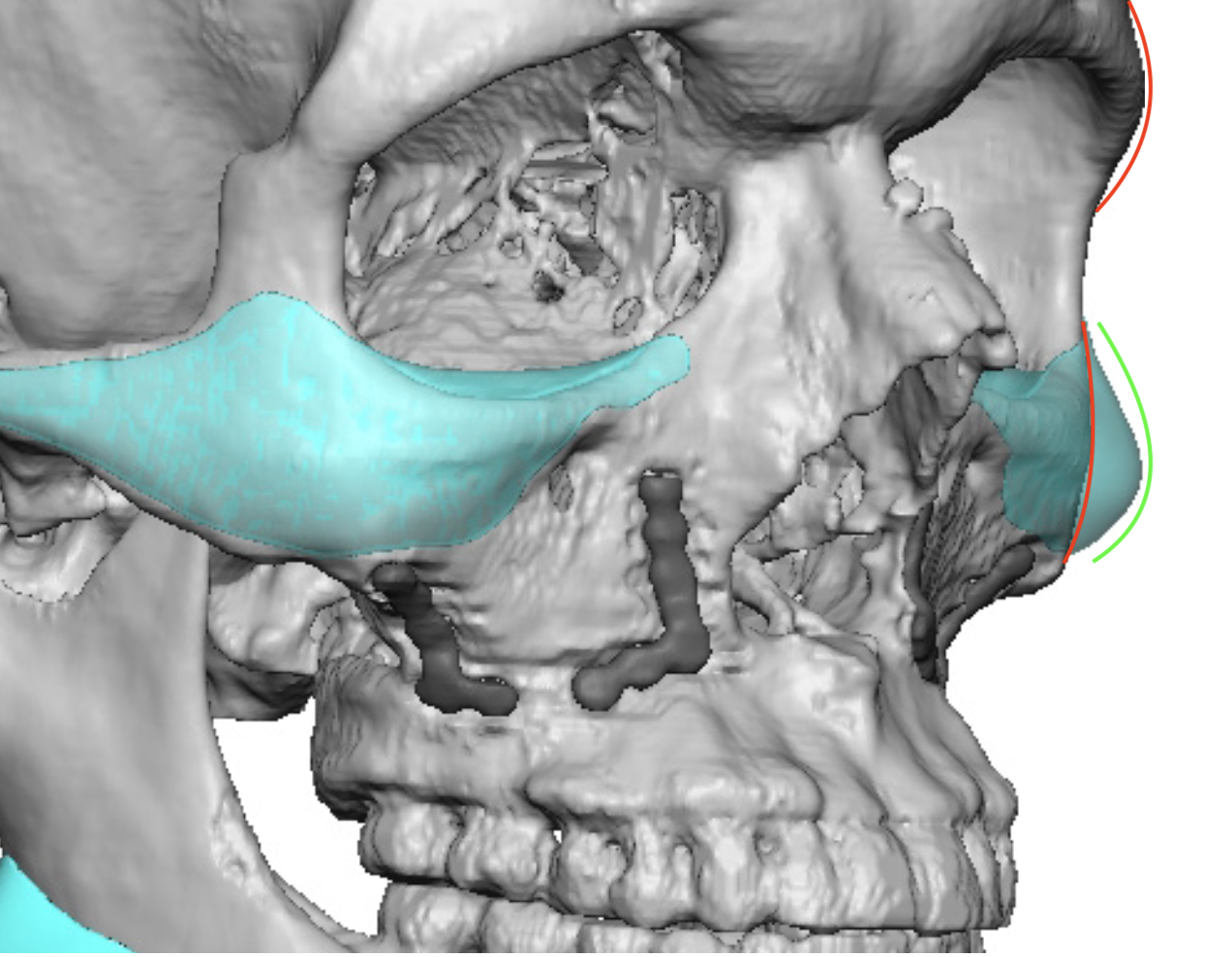
 One of the very important dimensions of the custom IOM implant is how it affects the Ogee curve. In this reverse S-shaped facial contour seen from the 3/4 view the projection of the cheek has a specific curved relationship to that of the brow bone. While almost always referred to as a desirable facial relationship in women it is rarely talked about how the Ogee curve relates to men. Whether it should be similar to that of women is up for debate and I don’t think they would be exactly similar. Males have naturally stronger brow bones projection at the tail and thus the upper part of the Ogee curve would naturally be more prominent. For the sake of proportion this would indicate that the cheek portion of the curve should be stronger as well. The cheek portion of the IOM implant should thus enhance the lower part of the Ogee curve which is usually too flat. Its projection can be less than, equal to or greater than a vertical line dropped down from the tail of the brow bone in the oblique view. It is best to think of these cheek projections as modest (less than), proportionate (equal to) or strong (greater than) which is a patient’s personal choice.
One of the very important dimensions of the custom IOM implant is how it affects the Ogee curve. In this reverse S-shaped facial contour seen from the 3/4 view the projection of the cheek has a specific curved relationship to that of the brow bone. While almost always referred to as a desirable facial relationship in women it is rarely talked about how the Ogee curve relates to men. Whether it should be similar to that of women is up for debate and I don’t think they would be exactly similar. Males have naturally stronger brow bones projection at the tail and thus the upper part of the Ogee curve would naturally be more prominent. For the sake of proportion this would indicate that the cheek portion of the curve should be stronger as well. The cheek portion of the IOM implant should thus enhance the lower part of the Ogee curve which is usually too flat. Its projection can be less than, equal to or greater than a vertical line dropped down from the tail of the brow bone in the oblique view. It is best to think of these cheek projections as modest (less than), proportionate (equal to) or strong (greater than) which is a patient’s personal choice.

 Proper placement of the IOM implant is often done ‘high’ through the lower eyelid as getting the correct horizontal line of implant placement is critical. The infraorbital section of the implant and its easy visibility through the lower eyelid incision usually ensures that the rest of the implant is in the correct location on the bone. It is really an implant that is ‘high and tight’ around the eye so to speak.
Proper placement of the IOM implant is often done ‘high’ through the lower eyelid as getting the correct horizontal line of implant placement is critical. The infraorbital section of the implant and its easy visibility through the lower eyelid incision usually ensures that the rest of the implant is in the correct location on the bone. It is really an implant that is ‘high and tight’ around the eye so to speak.
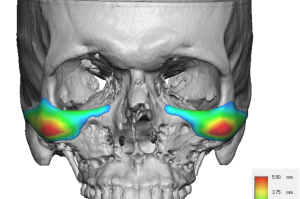 Looking at the implant on the bone in its design may seem like the augmentation is high but more careful inspection by looking at the color mapping of its thicknesses shows that its maximum projection is lower than one would think and is in line with the Ogee Curve assessment in the oblique view.
Looking at the implant on the bone in its design may seem like the augmentation is high but more careful inspection by looking at the color mapping of its thicknesses shows that its maximum projection is lower than one would think and is in line with the Ogee Curve assessment in the oblique view.
 One soft tissue procedure that may complement the custom IOM implant is the buccal lipectomy in some patients. Situated right below/under the cheekbone reduction of the buccal fat pad will create an increased concavity below the lower end of the cheekbone further enhancing the new prominence of the cheekbone. How much it will do so depends on the overall thickness of the patient’s soft tissue cover.
One soft tissue procedure that may complement the custom IOM implant is the buccal lipectomy in some patients. Situated right below/under the cheekbone reduction of the buccal fat pad will create an increased concavity below the lower end of the cheekbone further enhancing the new prominence of the cheekbone. How much it will do so depends on the overall thickness of the patient’s soft tissue cover.
Dr. Barry Eppley
World-Renowned Plastic Surgeon