

Breast implants are the second most common body contouring procedures behind liposuction and the most frequently performed implant placed in the body. As a result there is tremendous familiarity with breast augmentation surgery and its potential aesthetic effects. There is little question that the primary effect of breast implants is to make the breasts bigger. But the one potential effect that is often misunderstood is the effects such implants can have on a sagging breast.
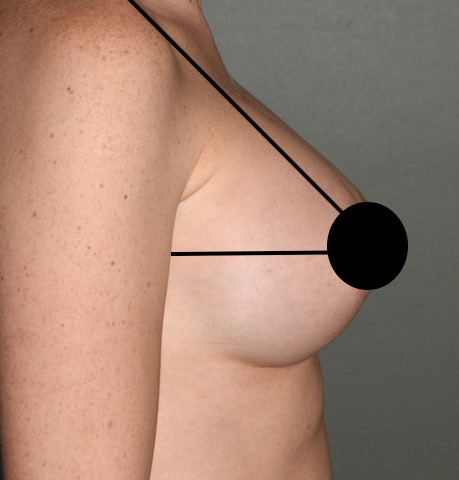
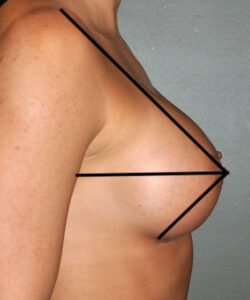 It is often assumed that the added volume of a breast implant can lift a sagging breast and this is true…up to a certain amount of sag. The rule of thumb is that as long as the nipple is above the inframammary fold an implant will lift the nipple higher. The nipple can even be as low as the actual inframammry fold and it will still be lifted. The position of the nipple on the mound is a reflection of how much loose breast skin exists. Thus it can also be seen that with enough implant volume even substantial loose breast skin can be filled and the nipple subsequently lifted. This can be best appreciated geometrically using a triangulation method in profile. One can see that as long as the lower limb of the triangle is horizontal, or nearly so, an implant will cause a breast lifting effect by volumetric expansion.
It is often assumed that the added volume of a breast implant can lift a sagging breast and this is true…up to a certain amount of sag. The rule of thumb is that as long as the nipple is above the inframammary fold an implant will lift the nipple higher. The nipple can even be as low as the actual inframammry fold and it will still be lifted. The position of the nipple on the mound is a reflection of how much loose breast skin exists. Thus it can also be seen that with enough implant volume even substantial loose breast skin can be filled and the nipple subsequently lifted. This can be best appreciated geometrically using a triangulation method in profile. One can see that as long as the lower limb of the triangle is horizontal, or nearly so, an implant will cause a breast lifting effect by volumetric expansion.
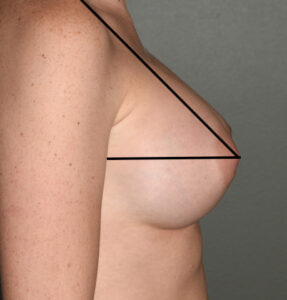
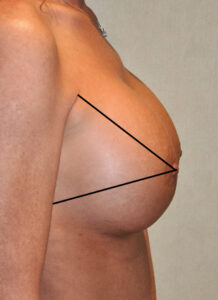 This is also illustrated in pseudoptosis (apparent breast sagging) where the nipple is at the level of the inframammary fold but breast tissue hangs below it. An implant will drive up the nipple with the added volume as well as pull the overhanging skin/breast tissue up with it.
This is also illustrated in pseudoptosis (apparent breast sagging) where the nipple is at the level of the inframammary fold but breast tissue hangs below it. An implant will drive up the nipple with the added volume as well as pull the overhanging skin/breast tissue up with it.
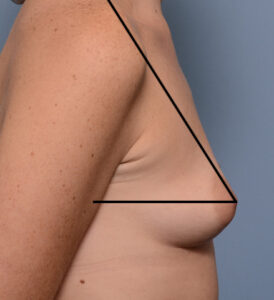
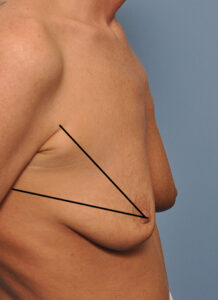
 But when the nipple is at or just below the inframammary fold (the triangle points downward) this is when the options in breast augmentation are less ideal. Such sagging is often not severe enough to warrant a formal breast lift with the resultant scars. And most patients would view such a tradeoff as undesirable particularly if they are younger. Options such as nipple and periareolar lifts exist, which produce a very modest and limited lifting effect, but such a limited lifting effect would usually be perceived as better than formal breast lift scars.
But when the nipple is at or just below the inframammary fold (the triangle points downward) this is when the options in breast augmentation are less ideal. Such sagging is often not severe enough to warrant a formal breast lift with the resultant scars. And most patients would view such a tradeoff as undesirable particularly if they are younger. Options such as nipple and periareolar lifts exist, which produce a very modest and limited lifting effect, but such a limited lifting effect would usually be perceived as better than formal breast lift scars.

 The tradeoff in this type of patient is that larger breast implants are needed and one has to accept a nipple position that will not be centric on the breast mound. And over time or with any weight gain the breast tissue is likely to slide off of the implants. The implants will remain in a fixed position but the breast tissue over it is not fixed. This will occur years later when one may be more willing to accept the breast lifting scars.
The tradeoff in this type of patient is that larger breast implants are needed and one has to accept a nipple position that will not be centric on the breast mound. And over time or with any weight gain the breast tissue is likely to slide off of the implants. The implants will remain in a fixed position but the breast tissue over it is not fixed. This will occur years later when one may be more willing to accept the breast lifting scars.

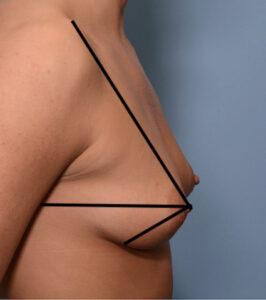
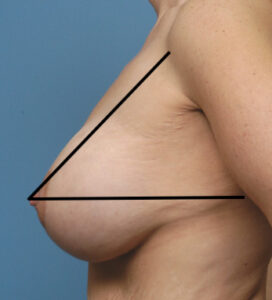 But when the nipple is pointing downward, and the horizontal limb of the triangle is more than a few degrees off from horizontal, the laxity and excess of breast skin is not enough to be overcome with any size breast implant. There is no equivocation that a breast lift is needed with the implant to right the breast triangulation shape.
But when the nipple is pointing downward, and the horizontal limb of the triangle is more than a few degrees off from horizontal, the laxity and excess of breast skin is not enough to be overcome with any size breast implant. There is no equivocation that a breast lift is needed with the implant to right the breast triangulation shape.
Dr. Barry Eppley
Indianapolis, Indiana