

Central midface augmentation refers to varying amounts of pyriform aperture implant coverages. The most common area is the paranasal region which lies under the base of the nostrils. This maxillary region has a slightly concave surface contour as a defined rim of bone around the nasal cavity. It is typically treated as a skeletal deformity most commonly due to midfacial hypoplasia using paranasal implants which have a long history of being composed of various materials and different shapes.

 Implants aside the paranasal region of the face is actually very commonly augmented by injectable fillers for what is usually age-related symptoms…the development of nasolabial folds. These well known skin folds develop as the soft tissue above the upper lip drift onto and over the lip-cheek junction. They are more prone to occur and develop deeper in flatter midface profiles due to lack of upper skeletal soft tissue support.
Implants aside the paranasal region of the face is actually very commonly augmented by injectable fillers for what is usually age-related symptoms…the development of nasolabial folds. These well known skin folds develop as the soft tissue above the upper lip drift onto and over the lip-cheek junction. They are more prone to occur and develop deeper in flatter midface profiles due to lack of upper skeletal soft tissue support.
Fillers are used to mask the depth of these folds which are always greatest by the side of the nose. Few think of the use of paranasal implants as a nasolabial fold implant rather than using injectable filler. But they can be very effective for the nasal component of deeper nasolabial folds as a solid push off of the bone outward on the soft tissues at the base of the nostrils..
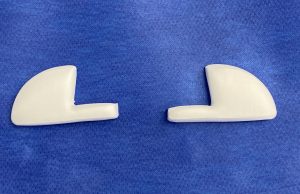
 There are numerous types of paranasal implants commercially available but my current preference is for ePTFE paranasal implants. The material allows for soft tissue adherence and this avoids the need for screw fixation. It also has a good shape to fit nicely around the pyriform aperture bone. It has enough lateral projection to get over into the canoe fossa region of the maxilla and its one arm can be removed or modified as needed.
There are numerous types of paranasal implants commercially available but my current preference is for ePTFE paranasal implants. The material allows for soft tissue adherence and this avoids the need for screw fixation. It also has a good shape to fit nicely around the pyriform aperture bone. It has enough lateral projection to get over into the canoe fossa region of the maxilla and its one arm can be removed or modified as needed.
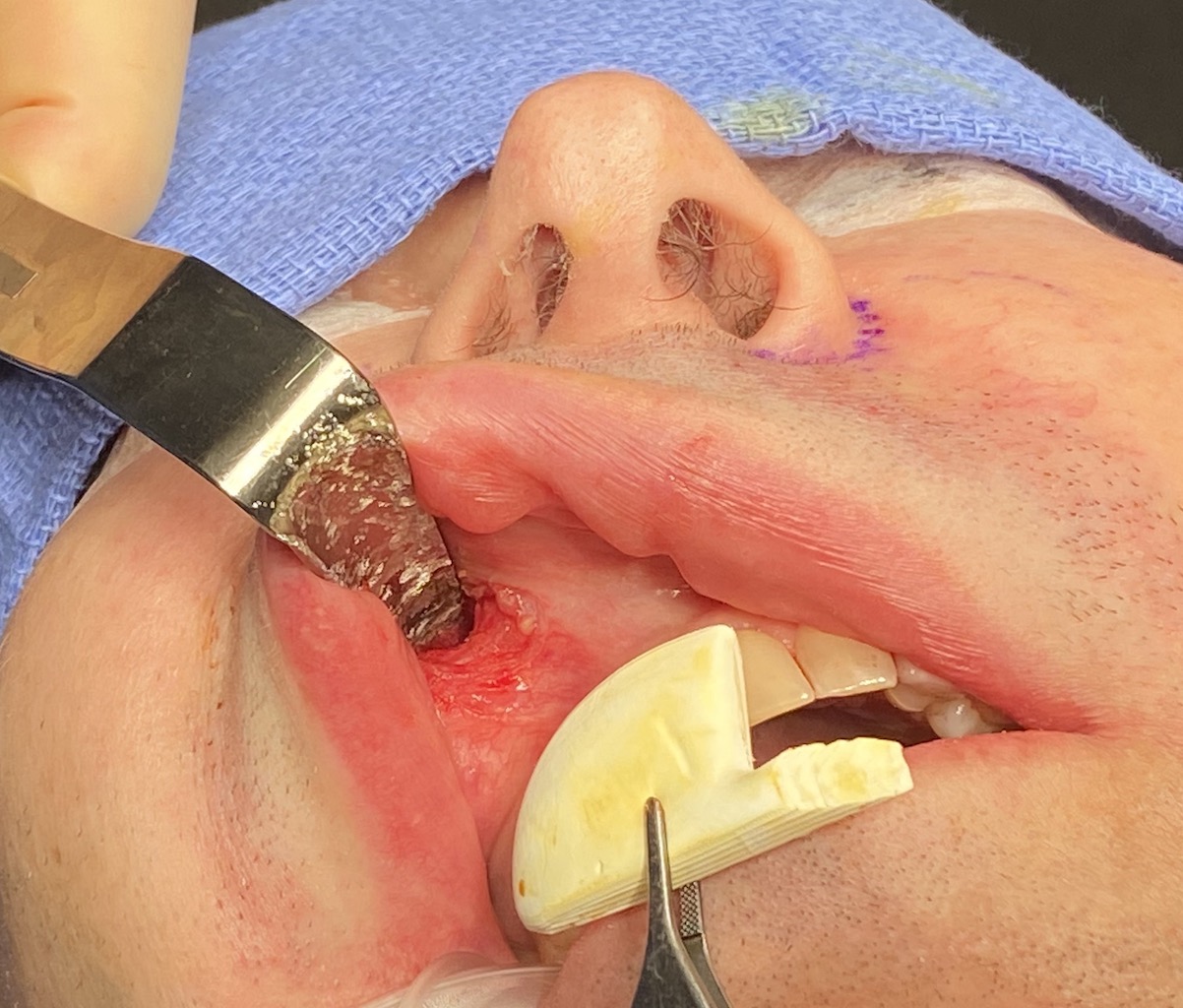
In the placement of paranasal implants the incision need not be very big and it needs to stay well above the mucogingival junction. It also needs to be high enough so a good muscle cuff is left on the inferior side of the incision for closure. Through this incision an adequate subperiosteal pocket can still be made. The size of the implant vs that of the incision may seem to be a mismatch but the implant will fit through it.

 The size of the subperiosteal pocket must be big enough so the implant can be maneuvered (turned) inside it to get the medial arm into position. Once properly placed I add some antibiotic powder and close the incision in two layers. (muscle and mucosa) It takes but a few dissolvable sutures to do so.
The size of the subperiosteal pocket must be big enough so the implant can be maneuvered (turned) inside it to get the medial arm into position. Once properly placed I add some antibiotic powder and close the incision in two layers. (muscle and mucosa) It takes but a few dissolvable sutures to do so.
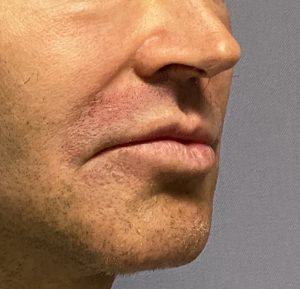
While the paranasal implant is intended to treat a midface hypoplasia and lack of nasal base projection, it can also be effective in the improvement of soft tissue-based deep overlying nasolabal fold. It works best in the nasolabial fold patient that also has a flatter mid facial profile where it can still look natural while improving both aesthetic hard and soft tissue deficiencies.
Dr. Barry Eppley
World Renowned Plastic Surgeon