


The precise origins of rib surgery for aesthetic waist contouring remain unclear. What is clear, however, is that the procedure has evolved significantly in philosophy, technique, and acceptance. Its progression can be divided into three distinct phases: early speculative removal, technique standardization, and modern structural modification.
 Phase I: The Era of Speculation (Pre-2010)
Phase I: The Era of Speculation (Pre-2010)
 Phase I: The Era of Speculation (Pre-2010)
Phase I: The Era of Speculation (Pre-2010)Prior to 2010, aesthetic rib removal was more myth than medicine. Frequently associated with celebrity rumors, the procedure lacked documentation in the surgical literature. Techniques were adapted from oncologic and trauma surgery, with the assumption that greater bone removal would yield greater contour change.
Operations typically involved complete excision of the free-floating 11th and 12th ribs through posterior incisions. While pleural complications were uncommon—since no ribs above #11 were removed—outcomes were unpredictable, and aesthetic results were not well characterized. Scar placement was posterior, and resections were aggressive.
This period was defined less by refinement and more by experimentation.
Typical Technique
- Complete excision of the free-floating 11th and 12th ribs
- Posterior (mid-back) incisions
- Full visualization of the rib during removal
Key Characteristics
- Limited to floating rib removal
- Aggressive resection
- Mid-back scar placement
What Was Learned
- Aesthetic outcomes and complication risks were largely unknown
- Low risk of pleural violation or pneumothorax because ribs above #11 were not removed
- Limited predictability of contour results
Phase II: Standardization and Validation (2010–2020)
 Phase II: Standardization and Validation (2010–2020)
Phase II: Standardization and Validation (2010–2020)The next decade marked a turning point. Aesthetic rib removal transitioned from rumor to reproducible technique. Subtotal resections of ribs 11 and 12 replaced complete excisions. Incisions became smaller and more laterally positioned. Rib #10 was incorporated in select cases, expanding contour potential.
Importantly, latissimus dorsi muscle reduction was introduced as an adjunct, recognizing that soft tissue contour contributes as much as skeletal structure to waist shape.
Clinical experience during this period demonstrated that rib removal could be performed safely, with low complication rates. However, aesthetic improvements proved patient-dependent. Structural modification produced measurable waist narrowing, but not always dramatic transformation. Skepticism within the broader plastic surgery community persisted.
What Changed
- Development of a more standardized surgical technique
- Better understanding of expected outcomes and risks
- Continued skepticism among many plastic surgeons regarding safety and effectiveness
Technical Modifications
- Subtotal resection of ribs 11 and 12 rather than complete excision
- Smaller, more limited posterolateral incisions
- Inclusion of rib #10 in selected patients
- Addition of latissimus dorsi muscle reduction to enhance contouring
What Was Learned
- Rib removal can be performed safely with very low complication rates
- Waistline improvement is achievable but varies significantly by patient
- Improved understanding of the anatomical relationship between rib modification and contour change
Phase III: Structural Contour Surgery (2020–Present)
 Phase III: Structural Contour Surgery (2020–Present)
Phase III: Structural Contour Surgery (2020–Present)Modern rib modification represents a shift from simple removal to strategic skeletal rand soft tissue eshaping.
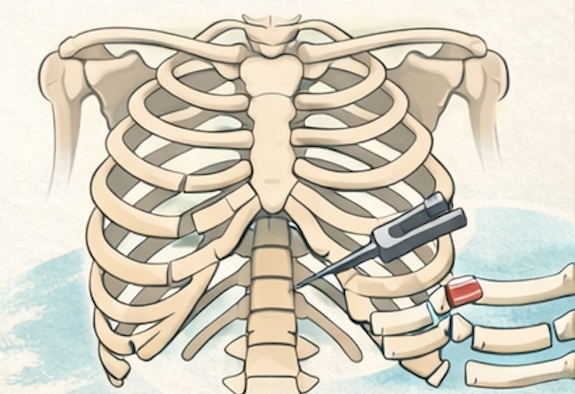
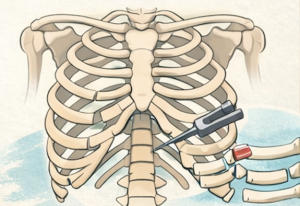
Recognition of rib #10 as a key contributor to torso width has led to standardized subtotal resections of ribs 10–12. More extensive latissimus reduction has enhanced contour beyond what rib modification alone can achieve.
Equally significant is the development of mijnimally invasive non-excisional techniques, including controlled rib fracture, which aims to alter rib projection while preserving structural continuity. Conversely more superior levels of ribcage modification by osteotomy shortening of ribs 8 and 9 has also been developed for those patients seeking higher levels of ribcage narrowing in 10 rib surgery reductions.
Rib modifications, whether minimally invasive or with aggressive removal techniques, is now frequently combined with liposuction, abdominoplasty, and hip or buttock augmentation as part of comprehensive contour strategies. While still not a first-line body contouring procedure for most patients, it is increasingly recognized as a legitimate adjunct in carefully selected cases.
Key Innovations
- Recognition of rib #10 as an important contributor to torso contour
- Standardization of subtotal resection of ribs 10, 11, and 12
- More extensive latissimus muscle reduction to enhance results beyond rib removal alone
- Introduction of non-excisional rib modification techniques (e.g., controlled rib fracture) through limited incisions
- Performance of rib modification in combination with other body contouring procedures (liposuction, abdominoplasty, buttock/hip augmentation)
- Increasing acceptance as a useful adjunctive contouring technique
- Osteotomy shortening of ribs 8 and 9 in select cases
Lessons Learned
 Lessons Learned
Lessons LearnedSeveral conclusions have emerged:
- Rib modification can be performed safely, with complication rates lower than many traditional body contouring procedures.
- Structural rib surgery produces real but not always dramatic contour change.
- Optimal outcomes depend on appropriate patient selection and combination approaches addressing bone, muscle, and fat.
- Long-term comparative data—particularly between excisional and non-excisional techniques—remain an important area for further study.
The Future of Aesthetic Rib Contouring
 The field continues to evolve toward greater precision. Emerging trends include 3D image-guided planning, hybrid contour strategies, expanded use of non-excisional reshaping, and long-term functional outcome tracking.
The field continues to evolve toward greater precision. Emerging trends include 3D image-guided planning, hybrid contour strategies, expanded use of non-excisional reshaping, and long-term functional outcome tracking.
Rib modification has matured from surgical folklore into a defined, technically nuanced procedure. Its future lies thoughtful structural ribcage changes integrated within comprehensive body contouring strategies.
Dr. Barry Eppley
Plastic Surgeon