

Temporal hollowing is often perceived as as sign of aging but also can occur due to genetics, disease or surgery. While the aesthetic interpretation of concave temporal areas is a personal one, many people prefer a more full temporal region. This could be making the temples less hollow or all the way to a convex contour based on the shape and proportions of the face below it.
While injectable fillers and fat injections are common non-surgical or minimally invasive temporal augmentation techniques, their permanency is not assured and often require multiple treatments for the effect to be maintained. A recently introduced silicone temporal implant offers a permanent temporal augmentation effect. Placed through a small vertical hairline incision and placed under the fascia, the temporal implant corrects temporal hollowing by adding volume to the muscle. This is unlike every other facial implant whose objective is to augment the underlying bone.
While standard temporal implants can very effectively improve temporal hollowing, their effects are relegated to the lower anterior temporal region by the side of the eye. This is where the deepest part of temporal hollowing occurs due to the shape of the temporal bone way below the skin surface. But the negative aesthetic effects of temporal hollowing can extend all the way up to the side of the forehead (anterior temporal line) which is beyond the augmentative effects of the standard temporal implant design.
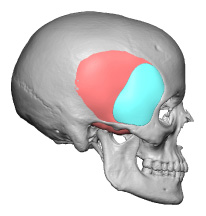
 For augmentation of the total anterior temporal region, a different temporal implant design is needed. The extended anterior temporal implant offers a design that extends from the zygomatic arch to the anterior temporal line vertically. It is thicker inferiorly and tapes into a fine edge at its superior extent. While every patient is different in size this new temporal implant is adequate for most patients with a lower thickness of 6mms.
For augmentation of the total anterior temporal region, a different temporal implant design is needed. The extended anterior temporal implant offers a design that extends from the zygomatic arch to the anterior temporal line vertically. It is thicker inferiorly and tapes into a fine edge at its superior extent. While every patient is different in size this new temporal implant is adequate for most patients with a lower thickness of 6mms.
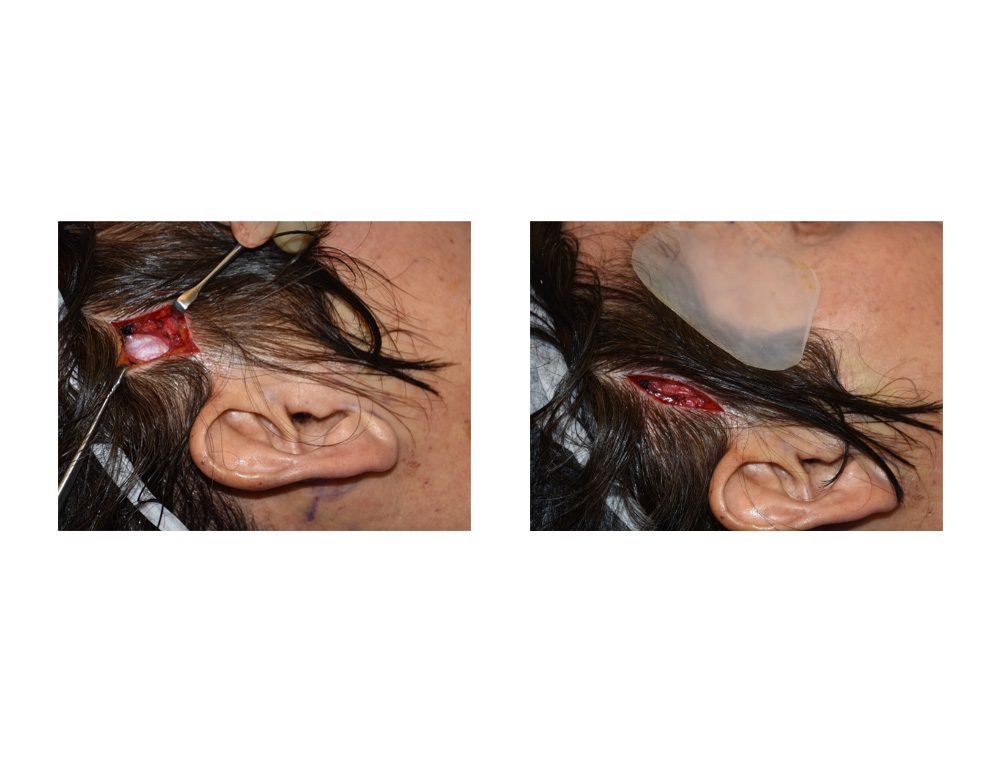
 The extended temporal implant is placed identically to that of the standard design. A small 4 cm vertical incision is made way back in the temporal hairline. This is usually above and behind the bifurcation of the temporal artery. The deep temporal fascia is found, incised and the implant pocket made bluntly and blindly. The pocket is developed based on preoperative markings of the desired areas of anterior temporal augmentation. The implant is inserted and placed beneath the deep temporal fascia and on top of the temporalis muscle.
The extended temporal implant is placed identically to that of the standard design. A small 4 cm vertical incision is made way back in the temporal hairline. This is usually above and behind the bifurcation of the temporal artery. The deep temporal fascia is found, incised and the implant pocket made bluntly and blindly. The pocket is developed based on preoperative markings of the desired areas of anterior temporal augmentation. The implant is inserted and placed beneath the deep temporal fascia and on top of the temporalis muscle.
By providing augmentation of the temporal region between the side of the forehead and the zygomatic arches, a more complete temporal augmentation is achieved. The larger extended anterior temporal implant is just as easy to place as the standard temporal implant. Clearly identifying the extent of temporal augmentation effect that a patient wants will allow one to choose the better implant design. It is often assumed by patients that the standard temporal implant provides an augmentation of the whole anterior temporal zone.
Dr. Barry Eppley
Indianapolis, Indiana