

The traditional tummy tuck (abdominoplasty) is primarily what I call a frontal approach where skin and fat is removed from the lower abdomen. The skin cutout is done horizontally in the shape of a football. Often times, liposuction is also performed on the sides around the waistline to get more of a 270 degree result. When the skin excess is not large, this is a perfectly fine approach and will immensely satisfy the vast majority of people who seek abdominal contouring.
When the amount of abdominal skin increases, however, the dimensions of the skin problem change. Redundant skin and fat is present not only in the horizontal direction but in the vertical dimension as well. Such abdominal problems exist in the larger abdominal pannus patient (skin overhang onto the thighs) and in the extreme weight loss patient. (greater than 100 lbs.)
If this additional dimension is not taken into consideration during the planning, patients may be disappointed with the result at the sides of the waistline. They may wonder why the side of the waistline does look as flat or as contoured as the front. Herein enters the concept of the extended tummy tuck, also known as the anchor tummy tuck or the fleur-de-lis tummy tuck.
 The extended tummy tuck adds a upper vertical cutout of skin along with the lower horizontally oriented skin removal. By so doing, the skin closure pulls in on the sides of the waistline as well as pulling down in the front. This effectively helps narrow the waistline as well and helps reduce the amount of redundant skin in that area. By adding this ‘third’ dimension to the tummy tuck, the length of the operation is increased but it does not result in any significant increase in the risk of postoperative problems.
The extended tummy tuck adds a upper vertical cutout of skin along with the lower horizontally oriented skin removal. By so doing, the skin closure pulls in on the sides of the waistline as well as pulling down in the front. This effectively helps narrow the waistline as well and helps reduce the amount of redundant skin in that area. By adding this ‘third’ dimension to the tummy tuck, the length of the operation is increased but it does not result in any significant increase in the risk of postoperative problems.
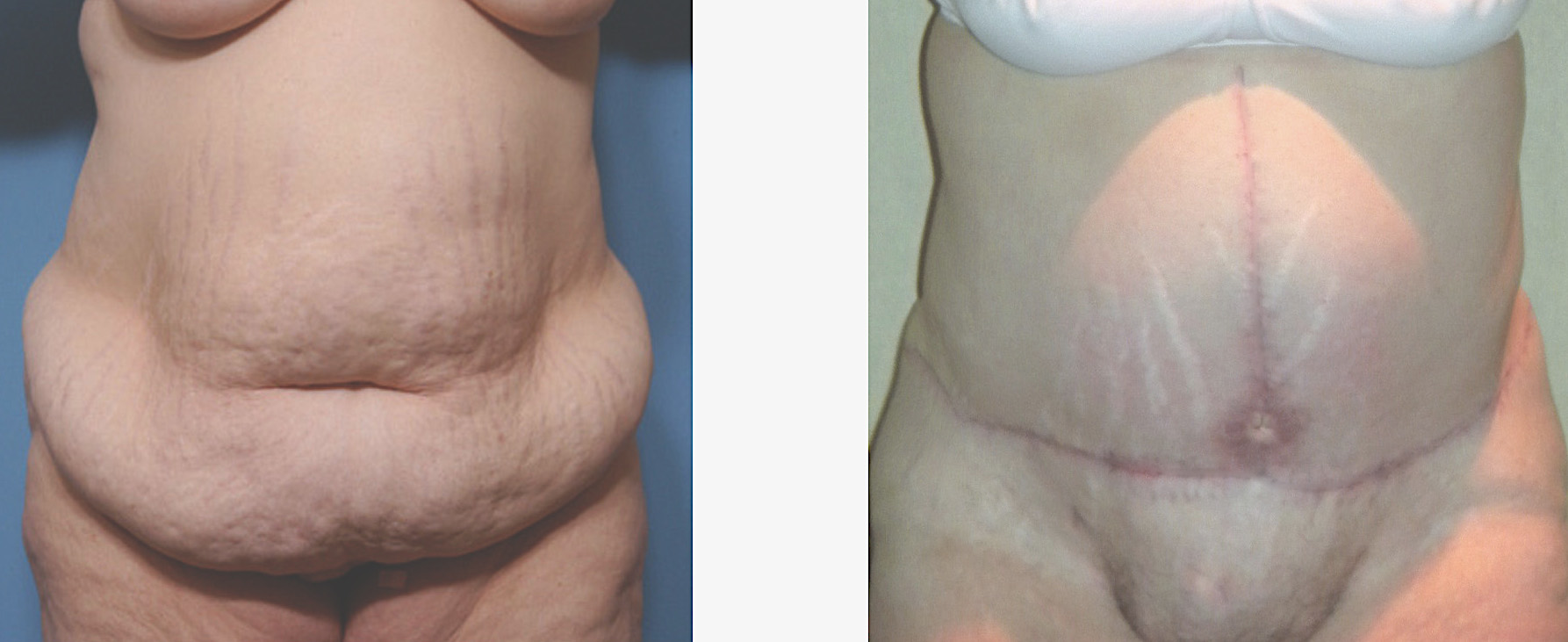 The extended tummy tuck (fleur-de-lis tummy tuck) does result in an additional scar that runs vertically from below the sternum down to the pubis. This creates the anchor scar result. Whether this extra scar is worth the trade-off for the improvement in the waistline is a personal choice. That choice is an easy one if an existing midline abdominal scar is already present. If no such midline scar exists, then one has to decide which ‘negative’ they can live with the best….loose skin on the sides or a vertical scar.
The extended tummy tuck (fleur-de-lis tummy tuck) does result in an additional scar that runs vertically from below the sternum down to the pubis. This creates the anchor scar result. Whether this extra scar is worth the trade-off for the improvement in the waistline is a personal choice. That choice is an easy one if an existing midline abdominal scar is already present. If no such midline scar exists, then one has to decide which ‘negative’ they can live with the best….loose skin on the sides or a vertical scar.
In my Indianapolis plastic surgery practice, I have noted that most patients with a lot of excess abdominal skin opt for the most skin removal and the best abdominal contour result. My general approach to the consideration of incisional scarring in non-hidden areas is…if you have to think about whether the scar is worth it…don’t do it. If the answer is an immediate yes and one could care less about the scar (compared to the existing problem), then the scar is not very likely to be a regrettable concern after surgery.
Dr. Barry Eppley
Indianapolis, Indiana