

Tummy tucks (abdominoplasty) traditionally are a horizontally-oriented operation. This means that excess skin and fat is removed with an elliptical incision that is oriented from one side of the waistline to the other. This results in a fairly low horizontal scar that is some distance below a newly created belly button. (if it is a full tummy tuck)
This conventional tummy tuck is effective for the vast majority of people as their abdominal skin excess is largely located in that direction. However, some patients have abdominal skin issues that have greater dimensional excesses than just in one direction. In my Indianapolis plastic surgery practice, I can determine this before surgery by looking at the sides of the waistline and seeing how much tissue bulges to the side. One can also see how much skin can be pinched in a vertical direction above the belly button.
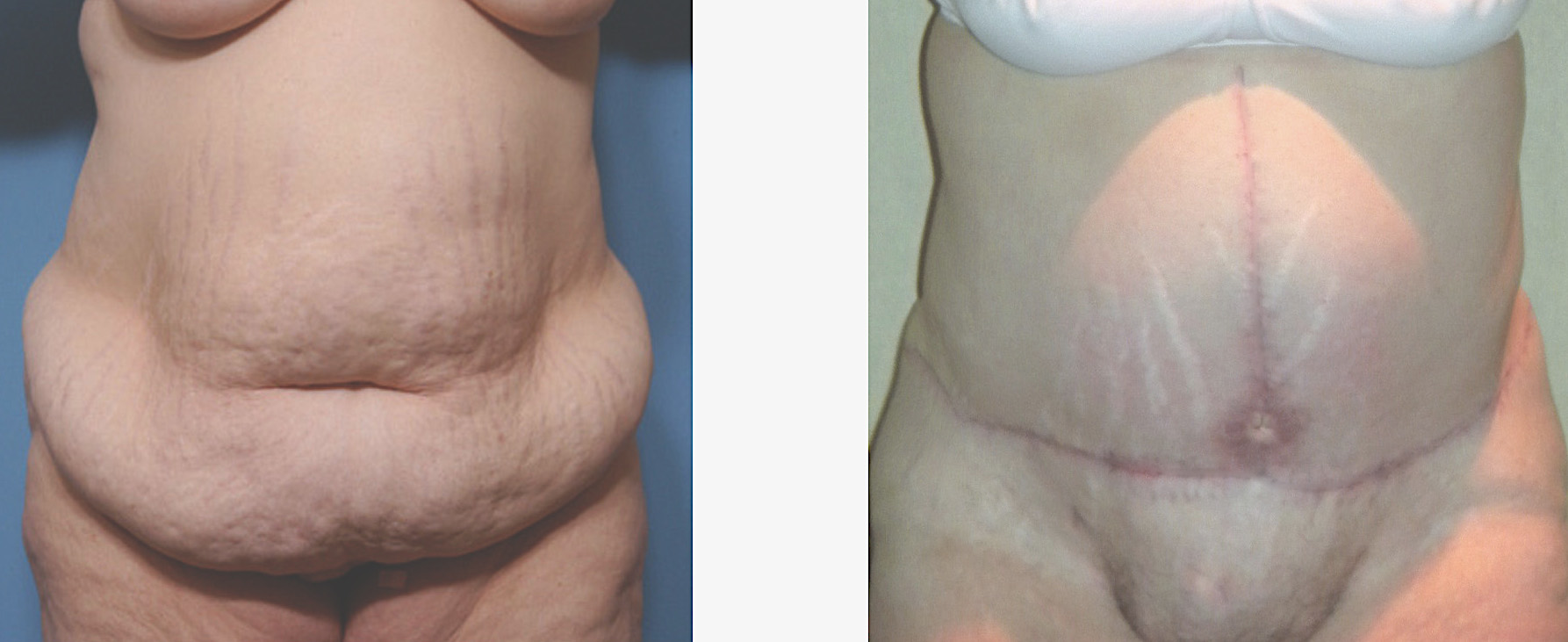 When there appears to be considerable vertical excess as well, consideration can be given to an extended or combined vertical-horizontal tummy tuck. This is also known as a fleur-de-lis type tummy tuck. By removing both horizontal and vertical tissue, the sides of the waistline are brought in as well as the frontal overhang removed. This creates a better abdominal result but there is a trade-off of a vertical closure as well as the horizontal one creating an anchor or inverted T scar.
When there appears to be considerable vertical excess as well, consideration can be given to an extended or combined vertical-horizontal tummy tuck. This is also known as a fleur-de-lis type tummy tuck. By removing both horizontal and vertical tissue, the sides of the waistline are brought in as well as the frontal overhang removed. This creates a better abdominal result but there is a trade-off of a vertical closure as well as the horizontal one creating an anchor or inverted T scar.
In the past, there were many more patients who presented with a history of prior abdominal surgery in which a midline scar was present. But the use of laparoscopic techniques is making such patients fewer and fewer. Therefore, the consideration of adding a vertical abdominal scar when one isn’t already present can be a difficult decision. If a vertical scar is present, however, the choice of an extended tummy tuck is straightforward.
While this type of tummy tuck always produces a better abdominal result, it does bring some increased risks of wound complications. The intersection of the vertical and horizontal closures at the inverted T creates a zone of tension. Combined with upper skin flaps that may have a blood supply to the skin edges which is compromised, it is not uncommon that these incisions can develop an opening at this intersection several weeks after surgery. This wound problem can be magnified based on where the new belly button is brought through on the vertical closure. Most of the time, this is only a few inches above the horizontal closure. These wound problems are self-limiting although it can take four to six weeks to close if the opening is significant.
Dr. Barry Eppley
Indianapolis, Indiana