

Asian patients are well known for the propensity for prominent cheekbones which creates a flatter and wider midface. This type of midface structure in the Asian patient can create a desire for less wide and more projected cheekbones. As a result a variety of cheek bone reduction osteotomies have been designed over the past four decades for this type cheekbone reshaping. SA form of facial bone surgery that is largely not known in Western patients who usually are seeking the exact opposite of cheek augmentation.
The original cheekbone reduction osteotomy, and one that is still used by some today, is a straight oblique cut line through the zygomatic body. More current modifications has been the L-shaped osteotomy pattern which offers a more three-dimensional reduction change to the cheek. But when the undesired width increase involves the lateral orbit neither the oblique or L-shape osteotomy pattern can address it.
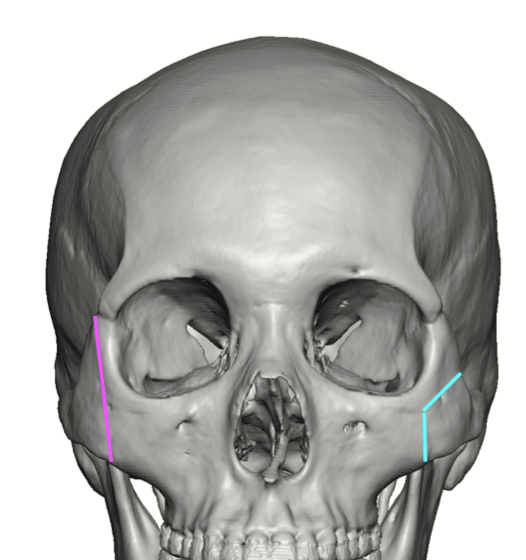
 In the February 2025 issue of Plastic and Reconstructive Surgery a paper on this topic was published entitled ‘Extended Reduction Malarplasty for Asians with Flat and Wide Faces: Comparison with L-Shaped Osteotomy.’ In this paper the authors used an extended L-shaped cheek osteotomy pattern that extend up into the lateral orbital wall in twenty patients over a two year period. Before and after CT scans were done to evaluate the bony changes between the standard (sLO) vs extended L-shaped osteotomy (eLO) patterns results.
In the February 2025 issue of Plastic and Reconstructive Surgery a paper on this topic was published entitled ‘Extended Reduction Malarplasty for Asians with Flat and Wide Faces: Comparison with L-Shaped Osteotomy.’ In this paper the authors used an extended L-shaped cheek osteotomy pattern that extend up into the lateral orbital wall in twenty patients over a two year period. Before and after CT scans were done to evaluate the bony changes between the standard (sLO) vs extended L-shaped osteotomy (eLO) patterns results.
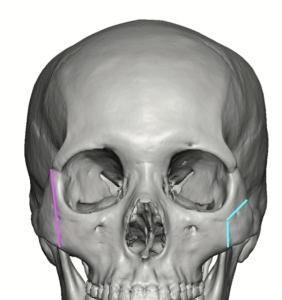
Cephalometric analysis between the two osteotomy patterns shows similar amounts of zygomatic width reductions. But only the eLO group showed significant improvement in the lateral orbital wall protrusion. In regards to facial angulation the eLO group provided more horizontal convexity in the periorbital area.
This study found that the eLO pattern enabled both reduction of the protrusion of the periorbital area and the prominent zygomatic body and arch. It alsomore 3-dimensionality and horizontal convexity with the midface contour.
Dr. Barry Eppley
World-Renowned Plastic Surgeon