

Shoulder feminization surgery reduces the bideltoid width through shortening of the length of the clavicles. While this is a straightforward concept as the lone horizontal bone on the body is the clavicle, doing so in an aesthetic manner requires several key steps to ensure an effective result that proceeds to uncomplicated bone healing and minimal scarring. Key steps are incision placement, amount of bone resection, bone stabilization and wound closure.

 The first step is proper incision location and length. This is based on the best location to shorten the clavicle which is at its inner third. The cross-sectional bone diameter is bigger here and it is also close to the stable sterno-clavicular articulation. This is also the location where the incision can be more hidden in the supraclavicular fossa up and behind the clavicle. The skin here is also a bit thinner which is another favorable feature for good scar healing. The length of the incision is no greater than 3.5cms. The skin incision serves as the ‘mobile window’.
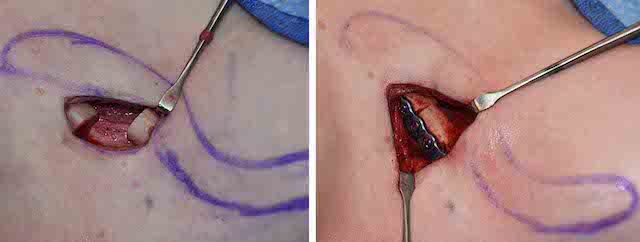
The first step is proper incision location and length. This is based on the best location to shorten the clavicle which is at its inner third. The cross-sectional bone diameter is bigger here and it is also close to the stable sterno-clavicular articulation. This is also the location where the incision can be more hidden in the supraclavicular fossa up and behind the clavicle. The skin here is also a bit thinner which is another favorable feature for good scar healing. The length of the incision is no greater than 3.5cms. The skin incision serves as the ‘mobile window’.

 Clavicle reduction technique 2 Dr Barry Eppley IndianapolsiCircumferential subperiosteal dissection exposes the medial clavicle in which 2.0 to 2.5cms of bone is removed. This has been shown for most patients to reduce their bideltoid width by 5 cms with medial and inward shoulder movement. It is not yet known how much more bone can be resected and still heal without increasing the risk of non-union or interfering with shoulder function. Clinical experience to date has shown this amount of bone resection to be both effective and leads to good bony unions.
Clavicle reduction technique 2 Dr Barry Eppley IndianapolsiCircumferential subperiosteal dissection exposes the medial clavicle in which 2.0 to 2.5cms of bone is removed. This has been shown for most patients to reduce their bideltoid width by 5 cms with medial and inward shoulder movement. It is not yet known how much more bone can be resected and still heal without increasing the risk of non-union or interfering with shoulder function. Clinical experience to date has shown this amount of bone resection to be both effective and leads to good bony unions.
 Plate fixation is essential in stabilizing the shortened clavicle length. Plate options are either 2.7mm or 3.5mm of which the lower profile 2.7mm plate and screws provide sufficient stability. When the contour of the bone permits the plate should be applied to the superior surface of the bone. This not only provides the best stability as shown in clavicle fracture repairs but also places the plate in a more non-palpable/visible location. Three bicortical screws of 12mm lengths on each side of the osteotomy are usually sufficient.
Plate fixation is essential in stabilizing the shortened clavicle length. Plate options are either 2.7mm or 3.5mm of which the lower profile 2.7mm plate and screws provide sufficient stability. When the contour of the bone permits the plate should be applied to the superior surface of the bone. This not only provides the best stability as shown in clavicle fracture repairs but also places the plate in a more non-palpable/visible location. Three bicortical screws of 12mm lengths on each side of the osteotomy are usually sufficient.

 Lastly wound closure is important to get a good soft tissue thickness/cover over the fixation plate. The periosteum on both sides of the clavicle should be found and closed over the bone and plate as the first layer. A second muscle layer of platysma is then closed followed by dermal sutures and a subcuticular closure. This provide a good thickness of soft tissue that makes the plate non-palpable at the end of the procedure.
Lastly wound closure is important to get a good soft tissue thickness/cover over the fixation plate. The periosteum on both sides of the clavicle should be found and closed over the bone and plate as the first layer. A second muscle layer of platysma is then closed followed by dermal sutures and a subcuticular closure. This provide a good thickness of soft tissue that makes the plate non-palpable at the end of the procedure.
By adhering to these key maneuvers in the procedure a successful aesthetic outcome can be achieved with a low rate of secondary scar revision or need for plate and screw removal.
Dr. Barry Eppley
Indianapolis, Indiana