

The latissimus dorsi (LD) muscle plays a significant role in aesthetic waist-narrowing rib surgery and affects how the procedure is performed as well as its aesthetic outcome.
Why the LD muscle is central to aesthetic rib removal
In aesthetic waist narrowing, the ribs of interest are almost always:
- 10th, 11th and 12th ribs
- Occasionally 8th and 9th ribs (rib shortening osteotomies)
 Anatomically, these ribs sit:
Anatomically, these ribs sit:
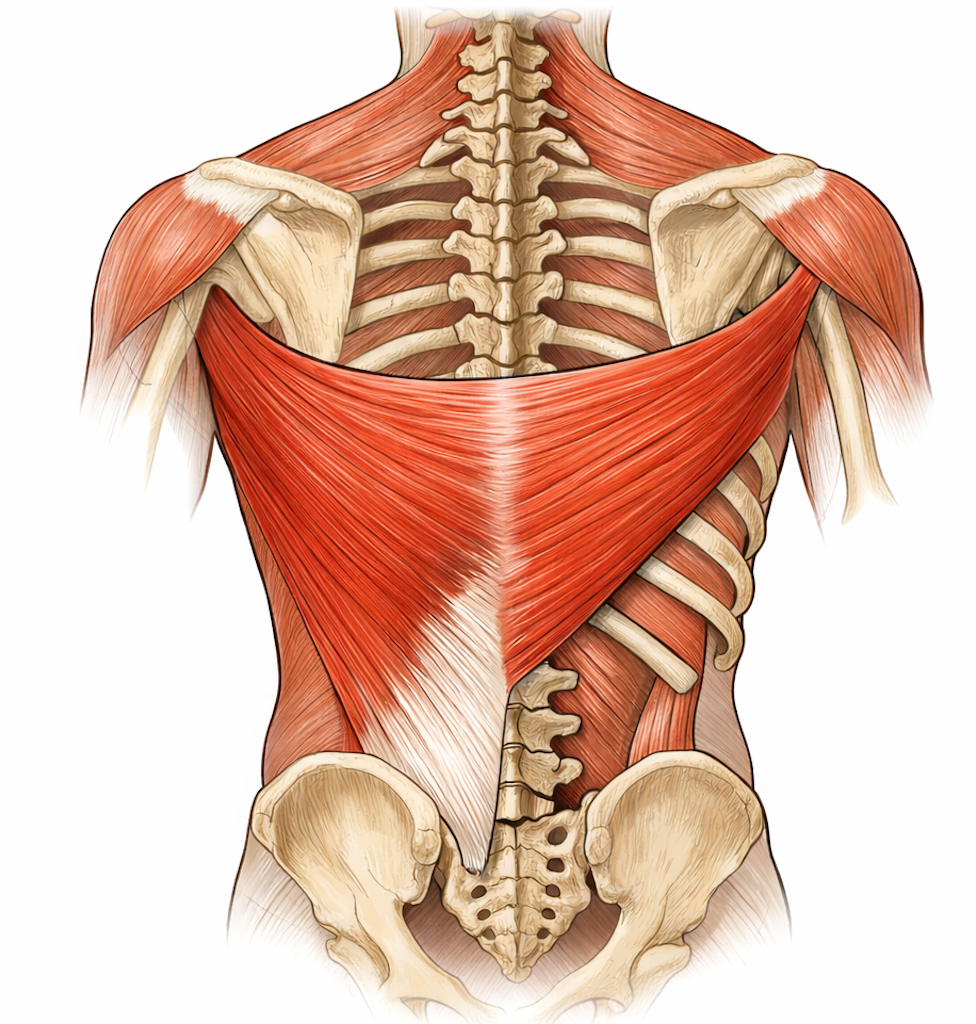
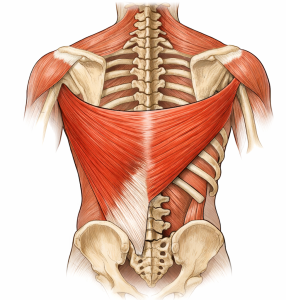
- Deep to the inferolateral portion of the latissimus dorsi
- Even the lowest rib, rib 12, lies deep and inside the outer border of the LD muscle
So the LD is:
- The primary muscle barrier
- A significant visual determinant of postoperative torso and waist contour
In other words, how the LD is handled directly affects the final waist shape.
LD Muscle Handling: Aesthetic Implications
Muscle splitting vs. muscle elevation
Preferred aesthetic technique
- Blunt splitting of LD fibers vertically well inside of the outer border (4 to 5cms inside)
- No transverse muscle cutting
- Limited muscle elevation medially, undermining laterally out to the outer muscle border
Why this matters:
- Preserves muscle bulk, avoids muscle atrophy/fibrosis which can occu from transverse muscle cutting
- Reduces dead space fluid collection/ibrosis that can “box out” the waist
- Maintains outer border shape, natural taper from ribcage to iliac crest
Alteration of LD Outer Border
Key landmark for waist definition as the outer edge of the LD:
- Often corresponds to the visible waist apex
- Impacts appearance/width of the lower ribcage
Rib removal alone may not always make the waist or lower ribcage look that much more narrow on its own
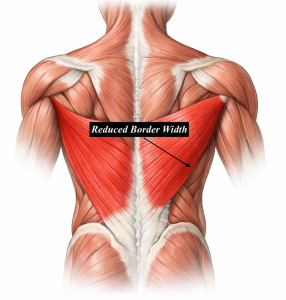 This is why LD width reduction improves the benefits of rib resection/ length shortening. It allows the structural rib changes to be more clearly seen.
This is why LD width reduction improves the benefits of rib resection/ length shortening. It allows the structural rib changes to be more clearly seen.
Is done after rib surgery is completed just prior to incisional closure
LD Muscle Width Reduction: Wedge vs Longitudinal Excision
Outer Width Reduction Technique:
 A V-shaped wedge excision is done perpendicularly at the visible waist apex at the lateral border
A V-shaped wedge excision is done perpendicularly at the visible waist apex at the lateral border- Prone to creating a more demarcated border indent depending upon the angles of the wedge excision
 A V-shaped wedge excision is done perpendicularly at the visible waist apex at the lateral border
A V-shaped wedge excision is done perpendicularly at the visible waist apex at the lateral borderInner Longitudinal Excision:
- An longitudinal elliptical excision is done along the split in the muscle used for rib access
- Closure of the excision pulls in the outer border of the muscle
- More aggressive outer border relocation can be pulling/plicating the remaining outer segment over and into the more fixed inner muscle section (preferred method)
- Maintains a smooth outer border of the muscle
- Changes the outer muscle border more effectively than the wedge technique
- The vertical incision provides a longer high to low muscle border alteraion than the oblique incisiion

 An longitudinal elliptical excision is done along the split in the muscle used for rib access
An longitudinal elliptical excision is done along the split in the muscle used for rib access The vertical incision provides a longer high to low muscle border alteraion than the oblique incisiion
The vertical incision provides a longer high to low muscle border alteraion than the oblique incisiionWhy LD matters here:
- The LD provides soft-tissue camouflage
- Its thickness smooths the transition from thorax to abdomen
- It prevents sharp contour breaks that read as “operated”
‘Conventional thinking has always made it out to be a bone surgery overlooking the soft tissue component of the ‘problem’’.
Bottom line
In waist-narrowing rib surgery, the LD muscle is:
- The gatekeeper to rib access
- The primary soft-tissue sculptor of the waist
- The camouflage layer that makes the result look more natural
- LD muscle border alteration (inward plication) is more important to do than removing an extra centimeter of rib
- Muscle redraping is complementary to bone absence for waist taper/more narrow torso
Dr. Barry Eppley
Plastic Surgeon