


Facial width reduction can be done by a variety of bone reshaping surgeries. Cheekbone osteotomies are a common techniques for reducing midfacial width. This is done by a combined anterior osteotomy done intraorally that goes through the main body of the zygoma and a posterior osteotomy done externally through the temporal process of the back end of the zygomatic arch. (or the zygomatic process of the temporal bone) This then allows the entire width of the cheekbones to be moved inward and stabilized with small plates and screws.
 For some patients their facial width concerns is only at the back end of the zygomatic arch. Their issue is the ‘bump’ that sticks out in front of their ears. This is actually the posterior zygomatic arch which in some people is the widest part of their zygomatic arch. It has more lateral protrusion than the anterior part of the arch as well as that of the temporal bone.
For some patients their facial width concerns is only at the back end of the zygomatic arch. Their issue is the ‘bump’ that sticks out in front of their ears. This is actually the posterior zygomatic arch which in some people is the widest part of their zygomatic arch. It has more lateral protrusion than the anterior part of the arch as well as that of the temporal bone.
 While often thought of as only part of an overall cheekbone reduction surgery, a posterior zygomatic arch osteotomy can be done as an isolated procedure to reduce this bump area. This is perform through a 1 cm vertical skin incision placed on the back end of the side burn hair. Blunt dissection is carrie through the subcutaneous tissues down to the bone to avoid the frontal branch of the facial nerve which does cross through this area. Once the posterior zygomatic arch is circumferentially isolated a reciprocating saw is used to make a beveled full-thickness bone cut.
While often thought of as only part of an overall cheekbone reduction surgery, a posterior zygomatic arch osteotomy can be done as an isolated procedure to reduce this bump area. This is perform through a 1 cm vertical skin incision placed on the back end of the side burn hair. Blunt dissection is carrie through the subcutaneous tissues down to the bone to avoid the frontal branch of the facial nerve which does cross through this area. Once the posterior zygomatic arch is circumferentially isolated a reciprocating saw is used to make a beveled full-thickness bone cut.

 An osteotome is used in front of the osteotomy cut to infracture the free end of the posterior arch inward. It can usually be moved at least 6 or 7mms. A 1.5mm plate is bent in the shape of a step and the outer end secured to the bone posterior to the bone with a single 1.5mm screw. The anterior end of the plate holds the fractured end of the bon inward. A screw in that portion of the plate is usually not needed as it blocks the bone from moving back outward.
An osteotome is used in front of the osteotomy cut to infracture the free end of the posterior arch inward. It can usually be moved at least 6 or 7mms. A 1.5mm plate is bent in the shape of a step and the outer end secured to the bone posterior to the bone with a single 1.5mm screw. The anterior end of the plate holds the fractured end of the bon inward. A screw in that portion of the plate is usually not needed as it blocks the bone from moving back outward.
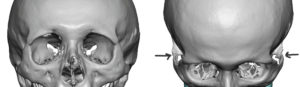
 It can be seen by 3D CT scan how effective the posterior zygomatic arch osteotomy is at removing the arch’s protrusion. The skin incision heals very well and is usually imperceptible at the side burn area.
It can be seen by 3D CT scan how effective the posterior zygomatic arch osteotomy is at removing the arch’s protrusion. The skin incision heals very well and is usually imperceptible at the side burn area.
 It is not uncommon that the posterior zygomatic osteotomy is combined with temporal reduction surgery to create a more complete face/head width reduction effect.
It is not uncommon that the posterior zygomatic osteotomy is combined with temporal reduction surgery to create a more complete face/head width reduction effect.
Dr. Barry Eppley
Indianapolis, Indiana