

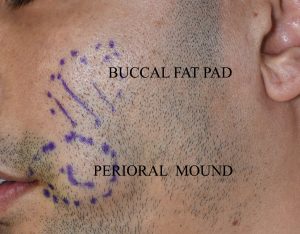
 The shape of the cheek area of the midface is influenced by a variety of anatomic structures, all of which are soft tissue in composition. This soft tissue makeup varies based on which level of the cheek one is addressing in what I refer to as the trampoline area, which is the soft tissue that lies between the bony cheeks and the bony jawline. From a surgical manipulation standpoint there are two specific cheek soft tissue regi0ns in the trampoline area that can be addressed/reduced. In the mid- cheek lies the buccal fat pad but in the lower cheek a bilaminar construct exists with an outside (skin and subcutaneous fat) and inside (muscle-mucosal) layers. Two fat removal procedures exist to address these areas which are the well known buccal lipectomy and the less well known perioral liposuction.
The shape of the cheek area of the midface is influenced by a variety of anatomic structures, all of which are soft tissue in composition. This soft tissue makeup varies based on which level of the cheek one is addressing in what I refer to as the trampoline area, which is the soft tissue that lies between the bony cheeks and the bony jawline. From a surgical manipulation standpoint there are two specific cheek soft tissue regi0ns in the trampoline area that can be addressed/reduced. In the mid- cheek lies the buccal fat pad but in the lower cheek a bilaminar construct exists with an outside (skin and subcutaneous fat) and inside (muscle-mucosal) layers. Two fat removal procedures exist to address these areas which are the well known buccal lipectomy and the less well known perioral liposuction.
Anatomically between the cheekbone and the jawline a muscle layer exists known as the buccinator muscle. It is a muscle that runs east-west and originates anteriorly from the alveolar processes of the upper and lower jaws. It extends back to the front edge of the pteryomandibular raphe. At its most anterior portion near the mouth the buccinator muscle fibers converge at the mouth corner with the circumferential orbicularis oris muscle. Given the location of its attachments contraction of the buccinator muscle pulls the corner of the mouth back and flattens the cheek inward. This serves as an assistive function in chewing to work in concert with the masticatory muscles.
From an aesthetic standpoint many younger patients desire a more inward or concave shape to their mid-cheek region between the cheek bones and the jawline. Some simulate this effect by sucking in their cheeks which is really activation of the buccinator muscle. Defatting procedures, such as buccal lipectomies and perioral liposuction, are the common procedures to try and create this facial reshaping effect. It is more successful in some than others. The thinner one’s face is the more successful those reductive cheek reshaping procedures are.


 But another potential procedure to help create that effect is a buccinator myectomy or muscle tightening done on the inside of the cheek on the either side of where perioral liposuction is done. Given that the muscle fibers run front to back, a partial resection and plication of a horizontal segment of the muscle located along a line at the level of the inside can help to make for a more inward outer cheek contour. This is done through an intraoral elliptical excision of mucosa, fat and muscle. Â This excision is done staying below location of the parotid duct.
But another potential procedure to help create that effect is a buccinator myectomy or muscle tightening done on the inside of the cheek on the either side of where perioral liposuction is done. Given that the muscle fibers run front to back, a partial resection and plication of a horizontal segment of the muscle located along a line at the level of the inside can help to make for a more inward outer cheek contour. This is done through an intraoral elliptical excision of mucosa, fat and muscle. Â This excision is done staying below location of the parotid duct.
There is no adverse functional sequelae from removing these small inner layers of the cheek. This is a technique that is borrowed from doing many buccal mucosal graft harvests for urethral reconstruction for Urologists in children and adults. The mucosal scar line heals wells and I never observed an adverse scar or infection. It also borrows somewhat from the concept behind cheek dimple surgery where reducing the muscular interface between the skin and mucosa is what creates the more localized cheek indentation
For those patients seeking a maximal effort in cheek reductive contouring buccinator myectomies is an option along with buccal lipectomies and perioral liposuction to maximize the effect.
Dr. Barry Eppley
Indianapolis, Indiana