

Adverse changes in the cheeks such as flatness and sagging is a common sequelae of aging as the tissues fall off of the cheekbones. Sagging cheek tissues combined with volume loss from fat atrophy make cheek management an important element of some facelift surgeries. Adding volume back and/or lifting of the cheeks back up can be done by a variety of methods including soft tissue rearrangement (SMAS flaps, deep plane facelift) and adding volume back through fat injection grafting or implants.
As a volume augmentation procedure for the cheeks it is understandable why fat injections are the primary method used by most surgeons. It is a natural replacement for the cheek volume lost, everyone has fat that can be harvested from somewhere, it is easy to inject and there are few complications with its use. Cheek implants, conversely, involve placement of an unnatural material, has a higher rate of complications than fat, and traditionally would require a new incisional approach than that of the facelift. (most commonly an intraoral approach) Despite these disadvantages cheek implants have two advantages over fat…assured volume retention and a better push on the overlying tissues due to its firmer structure. (better lifting effect)
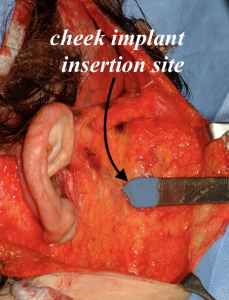 In the November 2022 issue of the journal an article was published on this topic entitled Zygomatic Implants through a Face-Lift Approach: Analysis of 30 Years Experience. In this paper the authors performed a retrospective review of 350 patients who underwent a facelift in which silicone cheek implants were placed through the same incisional (pre auricular) approach. They used a variety of cheek implant styles, malar shell and submalar, depending on the patient’s preoperative aesthetic cheek augmentation needs. Through a facelift approach a horizontal incision was made in the subcutaneous fat at the medial third of the zygomatic arch…an area where no nerve structures are located. Subperiosteal dissection is then done onto the cheekbone and out onto the masseteric fascia beyond the edge of the inferior cheekbone. Because of the narrow subperiosteal tunnel onto the bone the implant was folded for insertion and then unfolded once inside the pocket. Suture or screw fixation was not used. A single suture closed the small entrance incision opening into the subperiosteal cheekbone pocket.
In the November 2022 issue of the journal an article was published on this topic entitled Zygomatic Implants through a Face-Lift Approach: Analysis of 30 Years Experience. In this paper the authors performed a retrospective review of 350 patients who underwent a facelift in which silicone cheek implants were placed through the same incisional (pre auricular) approach. They used a variety of cheek implant styles, malar shell and submalar, depending on the patient’s preoperative aesthetic cheek augmentation needs. Through a facelift approach a horizontal incision was made in the subcutaneous fat at the medial third of the zygomatic arch…an area where no nerve structures are located. Subperiosteal dissection is then done onto the cheekbone and out onto the masseteric fascia beyond the edge of the inferior cheekbone. Because of the narrow subperiosteal tunnel onto the bone the implant was folded for insertion and then unfolded once inside the pocket. Suture or screw fixation was not used. A single suture closed the small entrance incision opening into the subperiosteal cheekbone pocket.
No cases of infection or implant displacement occurred. One hematoma developed and one case of temporay upper lip weakness occurred. Three patients (< 1%) developed implant seromas which were successfully resolved by aspiration. One implant was removed due to a chronic seroma that occurred from a dental infection.
Fat grafting was done in some patients, either doing the facelift (around the implants) or postoperatively for additional cheek volume over what the implants created.
 While fat grafting remains the primary method by which cheek augmentation is performed in facial rejuvenation (facelift) surgery, the use of cheek implants has largely been overlooked. This paper and the large number of patients done demonstrate that cheek implants can be safely placed through a preauricular facelift approach. There are always going to be a greater number of complications associated with an implant as opposed to fat injections but the numbers in this study were very low. This is not surprising given the avoidance of an intraoral incision. The main reason as the authors point out why cheek implants have a low rate of use in facelift surgery is that surgeons generally believe that is a more difficult and risky path of cheek implant placement… which this study shows is not the case.
While fat grafting remains the primary method by which cheek augmentation is performed in facial rejuvenation (facelift) surgery, the use of cheek implants has largely been overlooked. This paper and the large number of patients done demonstrate that cheek implants can be safely placed through a preauricular facelift approach. There are always going to be a greater number of complications associated with an implant as opposed to fat injections but the numbers in this study were very low. This is not surprising given the avoidance of an intraoral incision. The main reason as the authors point out why cheek implants have a low rate of use in facelift surgery is that surgeons generally believe that is a more difficult and risky path of cheek implant placement… which this study shows is not the case.
Dr. Barry Eppley
World-Renowned Plastic Surgeon