

The most recognized and common form of aesthetic facial surgery is that of facial rejuvenation. Typically performed on ‘older’ patients procedures such as facelifts, blepharoplasty and browlifts for example have been around for a hundred years and can ameliorate an inevitable concern that everyone will eventually face. While no patient really likes to undergo elective facial surgery, they do so with the expectation of looking and feeling better about their facial appearance. The early recovery period may be disturbing for some with the facial distortions that come from swelling and bruising. But the patient generally knows what the end point will be…a rejuvenated facial appearance that largely looks like a younger version of themselves. In essence they know where they are headed.
Another form of aesthetic facial surgery is that of facial reshaping surgery. Some of its procedures are very recognizable, rhinoplasty and chin augmentation for example, as they have been around for a long time. But in contemporary facial plastic surgery the number of facial reshaping procedures has expanded greatly to provide changes to a diverse ethnic and gender population around the world. Facial feminization and masculinization procedures offer a wide range of structural facial changes that strive to change how the face is perceived. The vast majority of these patients are younger than in facial rejuvenation surgery. But the one very significant difference is that the outcome of these surgeries is new as the shape of the face is being changed. In essence the patient can not be completely sure what they will look like and equally importantly how they will feel about it.
While long recognized and chronicled in rhinoplasty surgery, the psychological aspects of the outcome and the patient’s perception thereof can make for a troubling recovery period, patient unhappiness and numerous revisions surgeries. This is no less true for any form of facial reshaping surgery whether it be that of the chin, cheeks, forehead or jawline. Changing a young person’s facial shape is much more psychologically stressful than improving an older patient’s heavy eyelids or sagging neck.
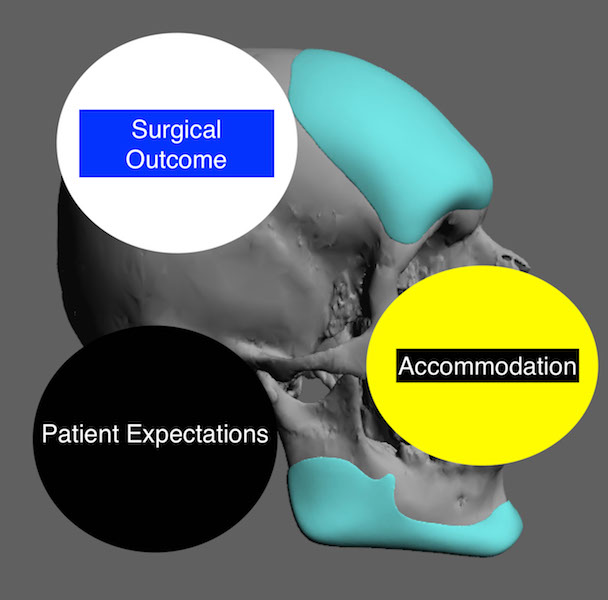
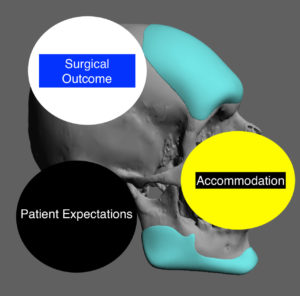 Despite computer imaging and extensive preoperative discussions with patients, the outcome of facial reshaping is never completely predictable. From a psychological standpoint the outcome is really a mix of three factors, patient expectations, the actual physical outcome and the patient accommodation or adjustment to it. Like a Venn diagram the more these three circles overlap or share common features the more likely the patient is to be satisfied.
Despite computer imaging and extensive preoperative discussions with patients, the outcome of facial reshaping is never completely predictable. From a psychological standpoint the outcome is really a mix of three factors, patient expectations, the actual physical outcome and the patient accommodation or adjustment to it. Like a Venn diagram the more these three circles overlap or share common features the more likely the patient is to be satisfied.
The tenuous nature of facial reshaping surgery is primarily driven by how well the patient can accommodate to the change. Having looked at one’s facial features for their whole life, changing its genetic shape can be more troubling for some patients than they initially thought. Just because one wants certain facial changes does not mean that they will sit well with these changes even if they may be very close to what they wanted to achieve. I have seen many patients who have achieved very good results but were not happy with them. Such unhappiness leads to revision surgery for which those outcome may still be unsatisfactory.
These concepts are particular relevant in custom facial implants where major facial shape changes can be created and the appeal of doing so by a specific implant design is alluring. Because no implant design can be assured preoperatively and implant designs are more easily changed than facial bones that have been modified the temptation for revisional surgery is magnified.
Dr. Barry Eppley
Indianapolis, Indiana