


Background
Neck sagging is an inevitable result of aging. The extent varies among individuals and is influenced by factors such as youthful neck shape and body weight. Strong jawlines with thinner tissues and healthy body weight tend to age with less noticeable neck changes, whereas those with less defined jawlines, thicker tissues, and higher body weights often develop a true “neck wattle.”
A neck wattle is a central accumulation of skin and fat that descends from the lower face and lateral neck toward the midline, where it hangs downward. Although not fully separated from deeper structures, it can feel as if it lifts away from the neck when grasped. Beneath it, there is typically subplatysmal fat and a widened platysmal gap, though the bulk of the wattle itself masks these anatomical issues.
The traditional and highly effective treatment for a sagging neck—including wattles—is a lower facelift (neck-jowl lift). This approach repositions loose tissues upward and backward toward the ear, allowing excess skin to be removed with scars placed in more discreet locations. However, some patients—such as older men with large wattles and significant medical histories—are not ideal candidates for facelifts. For these individuals, a direct necklift offers a simpler, lower-risk alternative by excising the wattle directly, with the tradeoff of a central neck scar.
Case Study
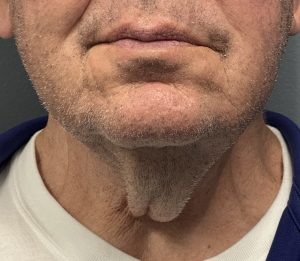 A 79-year-old male presented with a very large neck wattle. His medical history included cardiac ablation five years prior, and he was maintained on anticoagulation therapy. Given his medical risks, he elected for a direct necklift after multiple consultations regarding excision techniques, including variations with z-plasties.
A 79-year-old male presented with a very large neck wattle. His medical history included cardiac ablation five years prior, and he was maintained on anticoagulation therapy. Given his medical risks, he elected for a direct necklift after multiple consultations regarding excision techniques, including variations with z-plasties.
Preoperative Evaluation
 A pinch test was performed to estimate the necessary width of excision. Intraoperatively, the markings were revised to a slightly less aggressive plan, as the upright pinch test often overestimates tissue removal potential.
A pinch test was performed to estimate the necessary width of excision. Intraoperatively, the markings were revised to a slightly less aggressive plan, as the upright pinch test often overestimates tissue removal potential.
Surgical Technique
-
 Under general anesthesia, a central cutout within the original markings exposed the neck.
Under general anesthesia, a central cutout within the original markings exposed the neck. -
Subplatysmal fat was excised, and the widely split platysma was plicated at the midline.
-
The skin flaps were advanced medially and closed in an I-shaped pattern with fine resorbable sutures.
-
Closure sites were reinforced with adhesive tapes, serving as the sole dressing.
 Under general anesthesia, a central cutout within the original markings exposed the neck.
Under general anesthesia, a central cutout within the original markings exposed the neck. The skin flaps were advanced medially and closed in an I-shaped pattern with fine resorbable sutures.
The skin flaps were advanced medially and closed in an I-shaped pattern with fine resorbable sutures. Closure sites were reinforced with adhesive tapes, serving as the sole dressing.
Closure sites were reinforced with adhesive tapes, serving as the sole dressing.Postoperative Course
 The following day, the neck wattle was completely eliminated. As expected, the patient developed significant bruising in the lower neck, despite having discontinued anticoagulants several days before surgery.
The following day, the neck wattle was completely eliminated. As expected, the patient developed significant bruising in the lower neck, despite having discontinued anticoagulants several days before surgery.
Discussion
The direct necklift is particularly effective in older men—typically over 65 years—with large central wattles. Beard-bearing skin in the male neck heals surprisingly well, even with a central scar.
While some surgeons employ z-plasties to break up the midline closure or redistribute skin, I prefer a reverse hourglass excision pattern with continuous vertical closure. To avoid dog-ears, horizontal excisions are incorporated at the upper and lower ends of the vertical incision, resulting in an I-shaped closure. The lower horizontal cut is always larger and positioned along a natural crease above the sternal notch, maximizing reduction and ensuring smooth contour at both closure junctions.
Key Points
-
In older males with a large central neck wattle, the direct necklift is the most effective treatment option.
-
A reliable excision pattern involves upper and lower horizontal cuts with a bowed central excision, avoiding the need for z-plasties.
-
The wide-open access allows for subplatysmal defatting and midline platysmal plication, enhancing the result.
Dr. Barry Eppley
World-Renowned Plastic Surgeon