

There are multiple methods of jawline augmentation. Injectable fillers can be a good but temporary method which has its limitations long term due to economic reasons. But it can be a good initial test for some patients. The injection of fat, however, is frequently far less successful both due to its unpredictable survival but also due to an inability to create a well defined jawline.
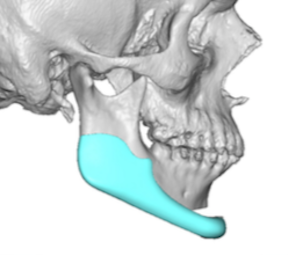
Permanent methods of jawline augmentation consist of four different mixtures of implants and osteotomies. The basic concept to grasp is that the chin can be changed by osteotomies or implants while the rest of the jawline can only be changed by implants. These potential combinations could be: 1) standard chin and jaw angle implants, 2) sliding genioplasty and standard jaw angle implants, 3) a total custom jawline implant, and 4) a sliding genioplasty with custom jawline implants.

 There are good reasons for each one of these methods and not all are best applied to everyone. The one that is least likely understood is the combination of a sliding genioplasty and custom jawline implants. The main reason to consider this option is when the amount of chin augmentation change is considerable. This could be based on the amount of pure horizontal movement or the combination of horizontal and vertical change needed.
There are good reasons for each one of these methods and not all are best applied to everyone. The one that is least likely understood is the combination of a sliding genioplasty and custom jawline implants. The main reason to consider this option is when the amount of chin augmentation change is considerable. This could be based on the amount of pure horizontal movement or the combination of horizontal and vertical change needed.
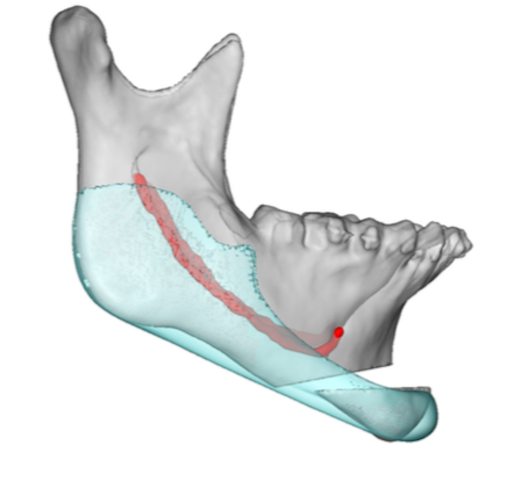
 The soft tissue chin pad is the tightest soft tissue along the jawline and often could be the thinnest as well. The greater the chin recession the thinner or less pliable the soft tissue chin pad can be which can be a limiting factor for implants. What you want to avoid is a large amount of implant load/stress on a soft tissue chin pad that is overly stretched out or closed under tension at the submental skin incision site. The safer strategy is then to do a sliding genioplasty which carries the soft tissue chin pad with it and maintains its vascularity over the maximal bony chin projection point by maintaining the soft tissue attachments.
The soft tissue chin pad is the tightest soft tissue along the jawline and often could be the thinnest as well. The greater the chin recession the thinner or less pliable the soft tissue chin pad can be which can be a limiting factor for implants. What you want to avoid is a large amount of implant load/stress on a soft tissue chin pad that is overly stretched out or closed under tension at the submental skin incision site. The safer strategy is then to do a sliding genioplasty which carries the soft tissue chin pad with it and maintains its vascularity over the maximal bony chin projection point by maintaining the soft tissue attachments.
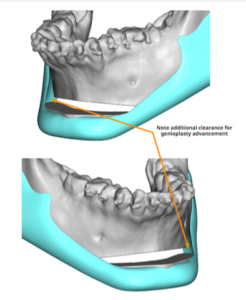 The question then becomes when does the amount of chin augmentation needed merit this combination as opposed to a total custom jawline implant. While there is no absolute proven number my experience is the when the horizontal chin augmentation exceeds 10 to 12mms in the horizontal direction or when the combination of horizontal and vertical is 14mms or greater then a sliding genioplasty should be done to lower the potential risks of complications. (infection, wound dehiscence)
The question then becomes when does the amount of chin augmentation needed merit this combination as opposed to a total custom jawline implant. While there is no absolute proven number my experience is the when the horizontal chin augmentation exceeds 10 to 12mms in the horizontal direction or when the combination of horizontal and vertical is 14mms or greater then a sliding genioplasty should be done to lower the potential risks of complications. (infection, wound dehiscence)
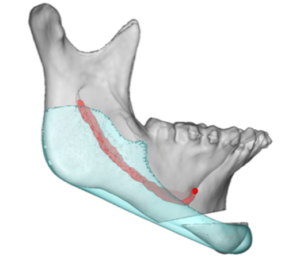
 When combining a sliding genioplasty and custom jawline implant there are two approaches. Have the sliding genioplasty do the majority of the chin augmentation and have the custom jawline implant complete it. Or have the sliding genioplasty do all of the chin augmentation and have the custom jawline implants only come up to merge along the sides of the chin and over the posterior osteotomy line/stepoff.
When combining a sliding genioplasty and custom jawline implant there are two approaches. Have the sliding genioplasty do the majority of the chin augmentation and have the custom jawline implant complete it. Or have the sliding genioplasty do all of the chin augmentation and have the custom jawline implants only come up to merge along the sides of the chin and over the posterior osteotomy line/stepoff.
Dr. Barry Eppley
Indianapolis, Indiana