


The most powerful form of aesthetic jaw augmentation is the custom jawline implant. It is so effective because it increases the dimensions of the entire jawline up to the limit of the overlying soft tissues in a three-dimensional fashion. The soft tissue limits are a function of how comfortably the implant fits into a fully released soft tissue pocket. (in other words can it be placed without compromising incisional closure or injuring surrounding vital structures)
How much the soft tissues can be stretched over an implant along the jawline is more limiting at the chin area than the jawline behind it. This is because the chin pad is the tightest soft tissue area of the entire jawline since it wraps around a solitary projecting bony point in the front. This creates limitations for implant size/fit in both the horizontal and vertical dimensions. In my experience I apply the rule of 12 to the chin area for implant fit…meaning any combination of horizontal and vertical millimeters increases that are needed beyond the cumulative number of 12 will be beyond what the the chin pad tissues can tolerate from implant expansion.
When the soft tissue pad can not tolerate the expansion needed for the chin part of the jawline implant the alternative strategy is to combine a bony genioplasty with the jawline implant. This is an autologous-alloplastic mixture of aesthetic jaw augmentation. A bony genioplasty can more safely tolerate large chin movements of any dimension whether it is horizontal, vertical or both. Ir does not have the same soft tissue limitation of implants particularly in the vertical dimension. (which requires the greatest soft tissue chin pad stretch)
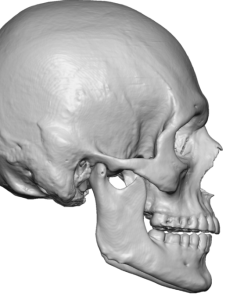
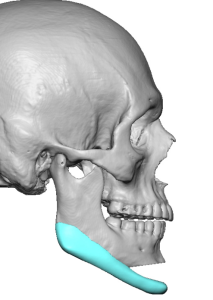
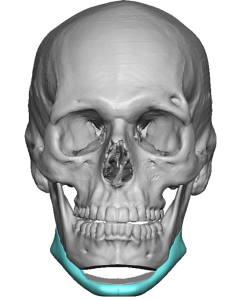 When designing a jawline implant when combined with a bony genioplasty both are created into the implant design file. The bony chin is first moved in the amount of horizontal and vertical increases that is needed and then the implant is designed around it. Even if the bony chin provides all the chin augmentation that is needed it is prudent for intraoperative implant placement to design the implant as a wrap around design.
When designing a jawline implant when combined with a bony genioplasty both are created into the implant design file. The bony chin is first moved in the amount of horizontal and vertical increases that is needed and then the implant is designed around it. Even if the bony chin provides all the chin augmentation that is needed it is prudent for intraoperative implant placement to design the implant as a wrap around design.

 The combo bony-implant jaw augmentation is done from a completely intraoral approach. The bony genioplasty is done first. If the bony movement is large enough, which it usually is when vertical lengthening is needed, an interpositonal cadaveric bone graft is usually needed to fill the gap. The custom jawline implant is then placed around it aided by additional posterior intraoral vestibular incisions.
The combo bony-implant jaw augmentation is done from a completely intraoral approach. The bony genioplasty is done first. If the bony movement is large enough, which it usually is when vertical lengthening is needed, an interpositonal cadaveric bone graft is usually needed to fill the gap. The custom jawline implant is then placed around it aided by additional posterior intraoral vestibular incisions.
The need for this type of aesthetic jaw augmentation is determined by preoperative facial picture imaging which determines the patient’s aesthetic goals. By looking at the amount of chin augmentation that the patient wants for their total jaw augmentation the choice of implant vs bony genioplasty is made. Very often the key lies in the amount of vertical lengthening as stretching the chin pad downward by an implant is limited.
Dr. Barry Eppley
World-Renowned Plastic Surgeon