


Rib removal is becoming a more well known procedure for waist narrowing. There are numerous methods for modifying the shape of the lower ribs to subtotal removal of them. But just as there are techniques to do it there are also specific types of patients who seek the procedure that require some modifications in technique to try and accomplish their goals.
One common patient that seeks rib removal is the transfemale. With a genetic torso shape that is wide throughout the entire ribcage the goal is to impact the lower torso as much as possible. Traditional (Type 1) rib removal/reshaping surgery is based on reduction of ribs #11 and #12 done through an oblique back incision whose goal is waistline reduction. While the waistline is defined as a circumferential line at the umbilical level the width issue goes higher up along the torso in the transfemale.
To help better address this aesthetic need it becomes important to get to rib #10 as well. Rib #10 is anatomically different from the two ribs below because it is attached. (sort of) It does wrap around the torso and joins the subcostal ribs anteriorly. But it does not truly attach and has a loose cartilaginous end right under rib #9. So a section of its wrap around portion can be removed for an increased narrowing effect. This also explains why rib fracturing does not work for rib #10 as breaking the bone posteriorly can not change its anterior position. Rib fracturing is based on the curve and distal end moving inward as its posterior bony attachment is loosened. This theoretically can work in a free floating rib with strong muscular attachments on its end.

 To more assuredly and safely treat rib #10 along with the two lower ribs the incision is changed to a more vertical orientation. This allows rib #10 to be well visualized. This has become known as Type 2 rib removals and is better suited to most transfemale needs. Starting at the lower end of the incision the distal end of rib #12 is removed.
To more assuredly and safely treat rib #10 along with the two lower ribs the incision is changed to a more vertical orientation. This allows rib #10 to be well visualized. This has become known as Type 2 rib removals and is better suited to most transfemale needs. Starting at the lower end of the incision the distal end of rib #12 is removed.
 One then works ‘up the ladder’ to rib #11.
One then works ‘up the ladder’ to rib #11.
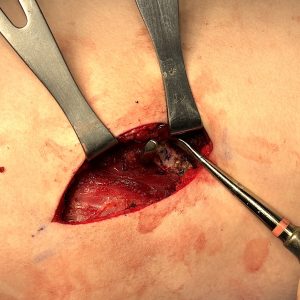
 At the top of the incision rib #10 is exposed and is immediately seen as different….bigger/wider and with harder to see clearly its superior surface. One must also be aware of the close proximity of the parietal pleura particularly on the right side. There is also the possibility of treating rib #9 by shaving it down very thin as opposed to total removal.
At the top of the incision rib #10 is exposed and is immediately seen as different….bigger/wider and with harder to see clearly its superior surface. One must also be aware of the close proximity of the parietal pleura particularly on the right side. There is also the possibility of treating rib #9 by shaving it down very thin as opposed to total removal.
The other advantage of the Type 2 incision is the ability to take a long and wide strip of the latissimus dorsi muscle which makes a significant contribution to the torso narrowing effort.
Dr. Barry Eppley
World-Renowned Plastic Surgeon