

There are various anatomic reasons for eye asymmetry most of which relate to the position of the eyelids to the globe…but the globes themselves are developmentally symmetric. But a very distinct form of eye symmetry is where the position of the globes themselves are not symmetric…one eye is at a different level than the other either vertically or horizontally. This is better termed am orbital asymmetry.
A distinct form of such eye asymmetry is vertical orbital dystopia. (VOD) In this congenital asymmetry the entire orbital box of one eye is at a different vertical level than the other. It may be higher or lower than the normal eye and it is up to the patient to say as to which is the normal eye. But in the vast majority of cases I have seen the abnormal eye is usually on the right side and is lower. (Right VOD)
What is unique about VOD and makes it challenging to surgically treat is that the entire orbital box is lower. This means every component of the eye and what surrounds it, the bony orbit, eyelids and eyebrow, is lower. As a result simply raising up the globe is not enough to improve the asymmetry and that maneuver alone may actually make it look worse.
A more effective and comprehensive approach to VOD surgery must take into account not only the position of the eyeball but that of the eyelids, brow bone, cheek and eyebrow as well. In my experience there are five layers to VOD surgery that often must all be done for an improvement in the eye asymmetry. The goal is two lessen the appearance of the asymmetry as complete improvement in the asymmetry is rarely if ever possible.
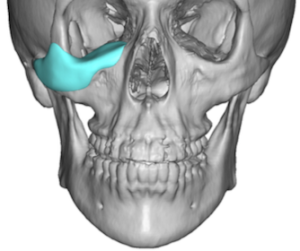
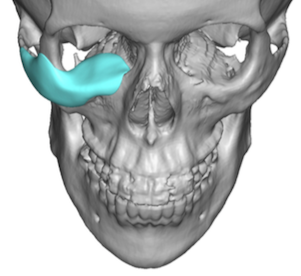 LAYER 1 The foundational approach in VOD surgery is the correction of the lower half of the orbital box and cheek. This is ideally done with a custom implant design based on the patient’s 3D CT scan. The implant is usually one piece which wraps around the infraorbital rim onto the orbital floor as well as extends out onto the cheek. By computer mirroring that of the opposite bony orbit an exact anatomic implant reconstruction can be made. As long as the amount of augmentation that is needed on the orbital floor does not exceed 5 mm the eyeball should be able to tolerate being pushed up. The implant portion on the rim provides additional support to the lower eyelid which also needs to be raised which is also assisted by that of the cheek correct as well.
LAYER 1 The foundational approach in VOD surgery is the correction of the lower half of the orbital box and cheek. This is ideally done with a custom implant design based on the patient’s 3D CT scan. The implant is usually one piece which wraps around the infraorbital rim onto the orbital floor as well as extends out onto the cheek. By computer mirroring that of the opposite bony orbit an exact anatomic implant reconstruction can be made. As long as the amount of augmentation that is needed on the orbital floor does not exceed 5 mm the eyeball should be able to tolerate being pushed up. The implant portion on the rim provides additional support to the lower eyelid which also needs to be raised which is also assisted by that of the cheek correct as well.
 The custom orbital-malar implant is always placed through a lower eyelid incision with a skin-muscle flap. Due to the size of the implant it is not usually possible to place it through a trans conjunctival incisional approach.
The custom orbital-malar implant is always placed through a lower eyelid incision with a skin-muscle flap. Due to the size of the implant it is not usually possible to place it through a trans conjunctival incisional approach.
 LAYER 2 the next step is then to address the lower eyelid reconstruction. The lower eyelid tissues are released and the lateral canthus repositioned up higher along the lateral orbital rim. This is most effectively done by a double hole lateral canthoplasty with a permanent suture.
LAYER 2 the next step is then to address the lower eyelid reconstruction. The lower eyelid tissues are released and the lateral canthus repositioned up higher along the lateral orbital rim. This is most effectively done by a double hole lateral canthoplasty with a permanent suture.
![]() LAYER 3 to help support and increase the height of the lower eyelid a spacer graft is beneficial. This is typically done with a cadaveric dermal graft such as Alloderm. Sewn in between the tarsus and the released orbicularis muscle the graft is extended out laterally up along the lateral orbital rim.
LAYER 3 to help support and increase the height of the lower eyelid a spacer graft is beneficial. This is typically done with a cadaveric dermal graft such as Alloderm. Sewn in between the tarsus and the released orbicularis muscle the graft is extended out laterally up along the lateral orbital rim.
LAYER 4 The lower eyelid is then closed by resuspending the cheek tissues up to the implant and the bony lateral orbital rim.
![]() LAYER 5 Most VOD patients will have a lower eyebrow as part of the more inferiorly located brow bone. As a result a brow lift is often needed. This can be done by a variety eyebrow lift techniques but one that is most convenient is the Endotine device method. It is convenient because it can be done through and upper eyelid incision with direct access for the release and lifting of the lower eyebrow. By placing the endotine device on the bone the eyebrow is then lifted and attached to the device. This is really a brow push technique rather than a superiorly lift-based technique that is more commonly done. But even if an endoscopic brow lift technique is used the upper eyelid incision provides an ideal method for a complete release of the lowered brow tissues.
LAYER 5 Most VOD patients will have a lower eyebrow as part of the more inferiorly located brow bone. As a result a brow lift is often needed. This can be done by a variety eyebrow lift techniques but one that is most convenient is the Endotine device method. It is convenient because it can be done through and upper eyelid incision with direct access for the release and lifting of the lower eyebrow. By placing the endotine device on the bone the eyebrow is then lifted and attached to the device. This is really a brow push technique rather than a superiorly lift-based technique that is more commonly done. But even if an endoscopic brow lift technique is used the upper eyelid incision provides an ideal method for a complete release of the lowered brow tissues.
LAYER 6 In some cases removal of the lower half of the brow bone may be beneficial if it is sufficiently lower than that of the opposite side. This is done with a high-speed handpiece and burr through the upper eyelid incision before the brow lift is completed.
LAYER 7 Lastly the upper eyelid position on the iris will usually need to be elevated as the eyeball has been pushed upward.. The elevation of the floor of the orbit will cause an iatrogenic ptosis. This is usually treated by multiple sutures placed between the tarsus and the levator aponeurosis. Well this is the easiest procedure to perform of all the VOD components it is the most difficult to get it just right given all the changes that have been performed around it and to know exactly how much lid elevation is needed in a patient who is asleep.
While some patients may need all seven layers of VOD surgery for optimal improvement some will not. The exact procedures needed will have to be decided on an individual basis based on the extent of VOD and how it has affected the surrounding tissues.
Dr. Barry Eppley
World-Renowned Plastic Surgeon