


Surgical jaw angle augmentation is most commonly associated with implants placed on the bone through an intraoral approach. These submuscular implants create their effect by extending the bony border of the ramus as well as pushing out the masseter muscle above it. It is this muscular effect that can create the need for a far less common type of jaw angle implant…one that does not go onto the bone under the muscle but on top of the muscle instead.
 This soft tissue jaw angle implant differs from its hard tissue cousin in numerous ways. Rather than used for bone augmentation it is intended instead to augment the soft tissues, specifically missing or deficient masseter muscle. Its use is to treat an adverse sequelae of bony jaw angle implant surgery that of masseter muscle dehiscence. This is a retraction of its ligamentous attachments to the jaw angle area due to surgical release for the placement of a bony implant. Once the ligamentous insertion has been released the muscle retracts (shortens) and the ability to ever surgically repair it is very limited. This creates a soft tissue contour deformity in the angle area of varying degrees. The most effective surgical treatment is a soft tissue implant to replace the missing muscle mass.
This soft tissue jaw angle implant differs from its hard tissue cousin in numerous ways. Rather than used for bone augmentation it is intended instead to augment the soft tissues, specifically missing or deficient masseter muscle. Its use is to treat an adverse sequelae of bony jaw angle implant surgery that of masseter muscle dehiscence. This is a retraction of its ligamentous attachments to the jaw angle area due to surgical release for the placement of a bony implant. Once the ligamentous insertion has been released the muscle retracts (shortens) and the ability to ever surgically repair it is very limited. This creates a soft tissue contour deformity in the angle area of varying degrees. The most effective surgical treatment is a soft tissue implant to replace the missing muscle mass.

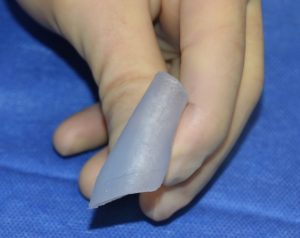 To more closely replicate muscle which it is intend to replace/augment, the implant is made of an ultra soft silicone material which is unlike the hard feel of bone.
To more closely replicate muscle which it is intend to replace/augment, the implant is made of an ultra soft silicone material which is unlike the hard feel of bone.
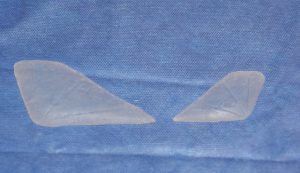 The implant dimensions are based on the exact shape, usually similar to a right angle triangle, of the soft tissue deficiency. Its thicknesses is whatever is needed to add the needed projection of the contour deformity. If the masseter muscle dehiscence is bilateral the dimensions will almost never be identical which is why they are custom made for each patient.
The implant dimensions are based on the exact shape, usually similar to a right angle triangle, of the soft tissue deficiency. Its thicknesses is whatever is needed to add the needed projection of the contour deformity. If the masseter muscle dehiscence is bilateral the dimensions will almost never be identical which is why they are custom made for each patient.

 The implant is placed through a small skin incision behind the area about 1 to 1.5cms in length. A precise deep subcutaneous pocket is created to the exact dimensions of the implant. The implant is inserted and the incision closed with small resorbable sutures. Trying to inset them from an incision around the earlobe or behind the ears often results in an implant placement that ends up too high.
The implant is placed through a small skin incision behind the area about 1 to 1.5cms in length. A precise deep subcutaneous pocket is created to the exact dimensions of the implant. The implant is inserted and the incision closed with small resorbable sutures. Trying to inset them from an incision around the earlobe or behind the ears often results in an implant placement that ends up too high.
Dr. Barry Eppley
World-Renowned Plastic Surgeon