

Shoulder width reduction is done by shortening the length of the clavicle by removing a segment of bone on each side. This collapse of the bone is achieved by a procedure known as clavicular reduction. It involves removal of a segment of bone through spaced osteotomies and an intervening ostectomy. The medial and lateral segments of the clavicle are then put back together with plate and screw fixation. While this concept for shoulder width reduction is straightforward, making it an acceptable aesthetic operation is all about the details of its execution. In theory it shares the basic details of clavicle fracture repair, but there are significant differences.
 The decision is to where the bone segment should be removed influences where the ideal incision location for the procedure is done. Removing a bone segment closer to the medial third of the clavicle places it in a location where the bone has a rounder cross-sectional shape. The bone is also a bit thicker in this area and its more even circumferential cortical thickness is most favorable for rapid bone healing. This allows the incision to be placed superior to this site in the supraclavicular fossa.
The decision is to where the bone segment should be removed influences where the ideal incision location for the procedure is done. Removing a bone segment closer to the medial third of the clavicle places it in a location where the bone has a rounder cross-sectional shape. The bone is also a bit thicker in this area and its more even circumferential cortical thickness is most favorable for rapid bone healing. This allows the incision to be placed superior to this site in the supraclavicular fossa.
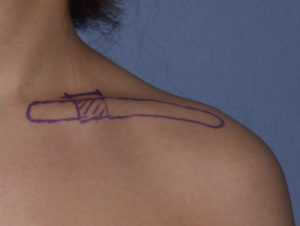
 The placement of the incision is of aesthetic significance. It is not placed directly over the bone which would be in the most visible location. Rather it is placed above the clavicle on the concave surface of the supraclavicuar fossa. This allows it to less visible in the shadow of the fossa. The length of the incision is remarkably short being no more than 3.5cms in length.
The placement of the incision is of aesthetic significance. It is not placed directly over the bone which would be in the most visible location. Rather it is placed above the clavicle on the concave surface of the supraclavicuar fossa. This allows it to less visible in the shadow of the fossa. The length of the incision is remarkably short being no more than 3.5cms in length.

 The incision, once made, is pulled up directly over the clavicle. Dissection is carried right down onto the bone where circumferential subperiosteal dissection is done. The spaced osteotomies are marked either 2 or 2.5cms apart. It is not yet known how much bone can be taken without affecting how it may heal or the stresses on it during healing. Clinical experiences has shown, however, that 2cms bone removal in each side creates a visible shoulder width reduction. More aggressive removal could be up to 2.5cms per side.
The incision, once made, is pulled up directly over the clavicle. Dissection is carried right down onto the bone where circumferential subperiosteal dissection is done. The spaced osteotomies are marked either 2 or 2.5cms apart. It is not yet known how much bone can be taken without affecting how it may heal or the stresses on it during healing. Clinical experiences has shown, however, that 2cms bone removal in each side creates a visible shoulder width reduction. More aggressive removal could be up to 2.5cms per side.

 With retractor protection the double osteotomy cuts are made and the bone segment is removed. With manipulation of the shoulder the length of the clavicle is shortened with approximation of the bone ends.
With retractor protection the double osteotomy cuts are made and the bone segment is removed. With manipulation of the shoulder the length of the clavicle is shortened with approximation of the bone ends.

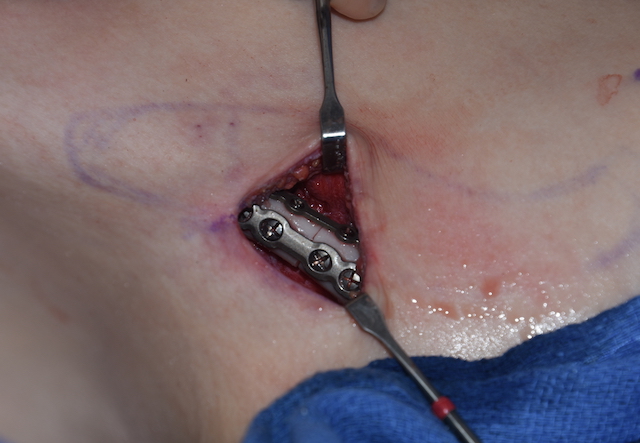
 Plate fixation of the clavicular reduction is done at done at its superior location where numerous biomechanics studies have shown to provide the best fixation. While traditional clavicle fracture repair uses 3.5mm plates, I use a 2.7mm plate with three bicortical screws per side. While probably adequate on its own I may supplement the fixation with a 2.0mm anterior plate with four monocortical screws to prevent any bone rotational concerns.
Plate fixation of the clavicular reduction is done at done at its superior location where numerous biomechanics studies have shown to provide the best fixation. While traditional clavicle fracture repair uses 3.5mm plates, I use a 2.7mm plate with three bicortical screws per side. While probably adequate on its own I may supplement the fixation with a 2.0mm anterior plate with four monocortical screws to prevent any bone rotational concerns.
 Multiple layer wound closure over the bone and plates is done with little to no palpability of the fixation hardware. Given their location it is not expected that the hardware will ever be seen or need to be removed after healing although this is always a possibility.
Multiple layer wound closure over the bone and plates is done with little to no palpability of the fixation hardware. Given their location it is not expected that the hardware will ever be seen or need to be removed after healing although this is always a possibility.
Shoulder width reduction using clavicular reduction osteotomy techniques is both visibly and aesthetically effective with the described surgical technique.
Dr. Barry Eppley
Indianapolis, Indiana