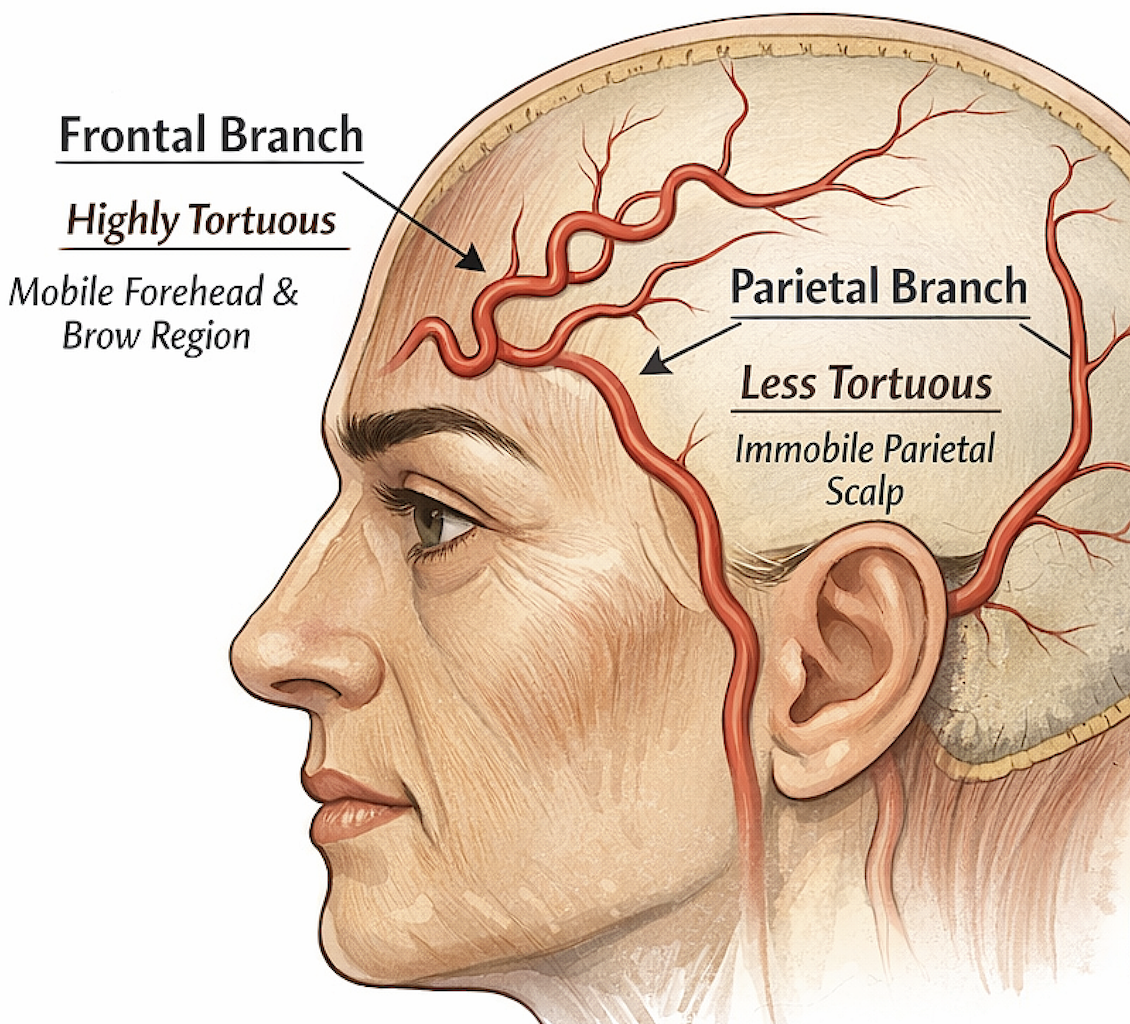


 The frontal branch of the superficial temporal artery (STA) is usually more tortuous than the parietal branch because of the greater mobility and dynamic activity of the forehead and brow region.
The frontal branch of the superficial temporal artery (STA) is usually more tortuous than the parietal branch because of the greater mobility and dynamic activity of the forehead and brow region.
1. High Mobility of the Forehead and Brow
The frontal branch supplies the forehead and anterior scalp, an area that moves constantly due to:
- Frontalis muscle contraction
- Eyebrow elevation
- Facial expression
- Blinking and periorbital movement
Because these movements repeatedly stretch and shorten the overlying soft tissues, the artery develops a serpiginous (wavy) configuration that acts like slack. When the forehead moves, the vessel can straighten slightly rather than stretch, protecting it from mechanical stress.
The parietal scalp, by comparison, is relatively immobile, so the parietal branch tends to be straighter.
2. Thin Soft Tissue and Lack of Muscle Cushion
In the temple–forehead transition zone, the artery runs:
- Within loose areolar tissue
- Over temporalis fascia
- In relatively thin soft tissue
This environment allows the vessel to shift position easily, which favors a tortuous course rather than a fixed straight one.
3. Developmental Lengthening
During growth, the forehead and anterior scalp expand considerably, particularly in childhood. The artery elongates with the soft tissue, and because the distance between its origin and distal distribution points is relatively fixed, the extra length often manifests as vascular tortuosity.
4. Pulsation and Superficial Location
The frontal branch is very superficial, making its pulsations more obvious. The wavy path accentuates this palpable pulse, which is why clinicians can often trace the artery with their fingers across the temple and forehead.
Surgical/Clinical Relevance
The increased tortuosity explains several practical observations:
- Forehead filler injections risk intravascular injection because the artery can wander unpredictably across the forehead.
- In temporal lifts or endoscopic brow lifts, the frontal branch can appear redundant and looping.
- In giant cell arteritis biopsy, the tortuous vessel is easier to identify and isolate.
Simple Mechanical Analogy
Think of the artery like a coiled phone cord:
- When the scalp stretches ? the artery straightens slightly
- When relaxed ? it returns to its serpiginous shape
This design prevents excessive tensile stress on the vessel wall.
If you’re interested from a plastic surgery perspective, there’s also a predictable zone where the frontal branch becomes most tortuous (about 1–3 cm above the zygomatic arch near Pitanguy’s line), which has implications for facelifts, temporal filler, and brow lift dissection.
there is a fairly predictable zone where the frontal branch of the superficial temporal artery (STA) becomes most tortuous, and it overlaps closely with the temporal danger zone defined by Pitanguy’s line. This has direct implications for facelift dissection, brow lifts, and temporal filler injections.
1. Location of the Tortuosity Zone
The maximal arterial redundancy typically appears:
~1–3 cm superior to the zygomatic arch
~1–2 cm anterior to the tragus
along or just anterior to Pitanguy’s line
Pitanguy’s line:
- From 0.5 cm below the tragus to 1.5 cm above the lateral eyebrow
This region represents the transition point where the STA divides into the frontal and parietal branches and where the frontal branch turns anteriorly toward the forehead.
At this turning point the artery commonly develops loops and serpiginous bends.
2. Why Tortuosity Occurs Here
Several mechanical factors converge at this location.
A. Directional Change of the Vessel
The frontal branch must change vector:
- Vertical ascent over the zygomatic arch
- ? Anterior sweep across the forehead
This turning point produces redundancy, which manifests as loops.
B. Frontalis Mobility
Just above the arch the vessel enters tissue that moves with:
- frontalis contraction
- brow elevation
- orbicularis oculi activity
Repeated motion encourages a serpiginous configuration that acts as a length buffer.
C. Superficial Tissue Plane
The frontal branch in this region lies in the:
subcutaneous plane just superficial to the deep temporal fascia
This relatively loose plane allows the vessel to wander, contributing to tortuosity.
3. Surgical Implications
Facelift (Temporal Dissection)
The most common site of STA injury during temporal dissection is 1–3 cm above the zygomatic arch.
Safe planes:
- Sub-SMAS inferiorly
- Deep temporal fascia plane superiorly
The artery often crosses the operative field in loops, making it vulnerable.
Temporal Filler
This is one of the highest-risk vascular zones in aesthetic injections.
Reasons:
- Vessel is superficial
- Loops unpredictably
- Can cross the injection trajectory multiple times
Safer approaches:
- Deep supraperiosteal injections
- Cannula use
- Avoid the Pitanguy line corridor
Brow Lift
During temporal endoscopic brow lift:
- The artery is encountered just superficial to deep temporal fascia
- Often seen looping across the dissection plane
Many surgeons preserve or cauterize it intentionally.
4. Practical Landmark Summary
|
Landmark |
Relationship |
|
Zygomatic arch |
Tortuosity begins 1–3 cm above |
|
Tragus |
About 1–2 cm anterior |
|
Pitanguy line |
Vessel runs along or just anterior |
|
Plane |
Subcutaneous / superficial to deep temporal fascia |
In short:
The most predictable zone of STA tortuosity occurs 1–3 cm above the zygomatic arch along Pitanguy’s line, where the vessel turns anteriorly into the mobile forehead. This region is therefore a key vascular danger zone for facelifts, brow lifts, and temporal filler injections.