

 Aesthetic upper eyelid surgery is primarily associated with the blepharoplasty procedure due to it being commonly performed. Whether for the removal of excessive upper eyelid tissues, the correction of a low hanging eyelid (ptosis repair) or the creation of a double eyelid, the supratarsal crease line is largely used for direct surgical access to perform these procedures. Despite its visibility it is a scar line that heals exceptionally well due to the thin tissues and its location in a naturally formed skin crease.
Aesthetic upper eyelid surgery is primarily associated with the blepharoplasty procedure due to it being commonly performed. Whether for the removal of excessive upper eyelid tissues, the correction of a low hanging eyelid (ptosis repair) or the creation of a double eyelid, the supratarsal crease line is largely used for direct surgical access to perform these procedures. Despite its visibility it is a scar line that heals exceptionally well due to the thin tissues and its location in a naturally formed skin crease.
The upper eyelid incision has also been used as a point of access for a variety of reconstructive surgeries. Orbital rim and cheekbone fractures, lacrimal gland suspension/removal, lateral canthoplasties and periorbital dermoid cyst removals in children are classic examples. When so used it is called the transpalpebral or through the eyelid approach.
But the transpalpebral approach has many other uses in aesthetic facial reshaping surgeries. Access for brow bone and forehead contour changes as well as eyebrow reshaping procedures can use this approach and avoid more distant points of access that have much longer incisional lengths. (e.g., hairline and coronal scalp incisions)
![]()
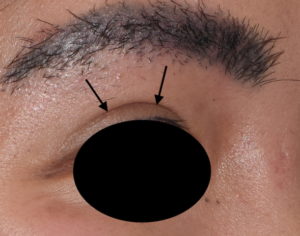
![]() The tail or temporal half of the brow bone can be reduced/reshaped using the transpalpebral approach. For the transgender male to female patient who has undergone a prior brow bone reduction but the outer brow has been overlooked or inadequately reduced, the upper eyelid provides a more direct and less invasive approach. This is also applicable for the cis-female who has lateral brow bones that are too prominent.
The tail or temporal half of the brow bone can be reduced/reshaped using the transpalpebral approach. For the transgender male to female patient who has undergone a prior brow bone reduction but the outer brow has been overlooked or inadequately reduced, the upper eyelid provides a more direct and less invasive approach. This is also applicable for the cis-female who has lateral brow bones that are too prominent.
![]() In aesthetic vertical orbital dystopia where the brow bone is lower on one side because of the inferior positioning of the entire orbital bony box, removing the lower edge of the brow bone is helpful. This is usually done in conjunction with orbital floor augmentation.
In aesthetic vertical orbital dystopia where the brow bone is lower on one side because of the inferior positioning of the entire orbital bony box, removing the lower edge of the brow bone is helpful. This is usually done in conjunction with orbital floor augmentation.
 In the converse of tail of the brow bone reshaping, augmentation can similarly be done though the transpalpebral approach with bone cements. For modest and isolated lateral brow bone augmentation, hydroxyapatite cements can be applied.
In the converse of tail of the brow bone reshaping, augmentation can similarly be done though the transpalpebral approach with bone cements. For modest and isolated lateral brow bone augmentation, hydroxyapatite cements can be applied.
![]() In the placement of custom brow bone implants, particularly those that have a significant lateral orbital rim extension, adding an inferior transpalpebral approach with a superior endoscopic technique is invaluable. Getting the thinner lateral orbital rim ‘tails’ down into the correct position is not easy or assured from a superior endoscopic approach alone. Besides positioning the transpalpebral approach allows direct small screw fixation of the orbital rim extensions with more assurance about their positioning.
In the placement of custom brow bone implants, particularly those that have a significant lateral orbital rim extension, adding an inferior transpalpebral approach with a superior endoscopic technique is invaluable. Getting the thinner lateral orbital rim ‘tails’ down into the correct position is not easy or assured from a superior endoscopic approach alone. Besides positioning the transpalpebral approach allows direct small screw fixation of the orbital rim extensions with more assurance about their positioning.
![]() In temporal browlift surgery, particularly when a significant tail of the brow elevation is desired, the transpalpebral approach allows the bets method for a complete subperiosteal release of the outer half of the eyebrow soft tissues. Such temporal browlifts are often done with with brow bone remodeling as well.
In temporal browlift surgery, particularly when a significant tail of the brow elevation is desired, the transpalpebral approach allows the bets method for a complete subperiosteal release of the outer half of the eyebrow soft tissues. Such temporal browlifts are often done with with brow bone remodeling as well.
![]() In the male browlift which is limited by lack of adequate hair for any of the more traditional browlift techniques, a transpalpebral approach allows an inferior-based brow release with placement of the endotine device for brow elevation. This approach produces only a modest browlift effect which is appropriate for most older men where over correction is the biggest aesthetic concern.
In the male browlift which is limited by lack of adequate hair for any of the more traditional browlift techniques, a transpalpebral approach allows an inferior-based brow release with placement of the endotine device for brow elevation. This approach produces only a modest browlift effect which is appropriate for most older men where over correction is the biggest aesthetic concern.
The transpalpebral approach is a valuable point of access for numerous facial reshaping procedures. While it is commonly believed that most changes around the brow bone and lateral orbital rim area can be achieved with a superior endoscopic approach, this is not accurate particularly when it comes to bone reduction/augmentation changes. But is also provides a more complete soft tissue release for certain types of temporal browlifts, particularly in those women who desire a more extraordinary type of change.
Dr. Barry Eppley
Indianapolis, Indiana