


The concept of rib removal for waistline reduction is based on removing parts of the lower bony ribcage to allow the sides of the waistline to collapse inward. When looking at the length and angulation of ribs #11 and #12 in particular it is easy to appreciate how this effect can occur. As attached to these ribs, which flare out from their attachments to the spine, are various abdominal wall muscles which lose this support when removed.
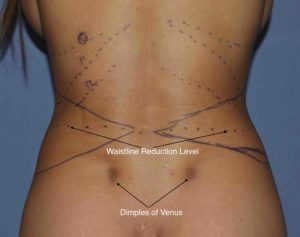
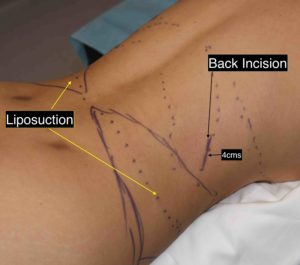 But having performed many rib removal surgeries, it is a procedure that has evolved over time of which the name belies the extent the more complete anatomic approach that is taken to surgical waistline reduction. The basic rib removal surgery includes flank liposuction, subtotal rib removals and latissimus dorsi muscle reduction. In marking the patient before surgery the location of the flank liposuction is marked with a lateral triangular pattern of which the optimal circumferential waistline reduction level usually comes across its middle. They access for the liposuction is the Dimples of Venus marks on the lower back which in some patients are very accentuated.The location of the incisions for the internal tissue removals is placed to the side of the back located over rib #11. The incision length is 4cms.
But having performed many rib removal surgeries, it is a procedure that has evolved over time of which the name belies the extent the more complete anatomic approach that is taken to surgical waistline reduction. The basic rib removal surgery includes flank liposuction, subtotal rib removals and latissimus dorsi muscle reduction. In marking the patient before surgery the location of the flank liposuction is marked with a lateral triangular pattern of which the optimal circumferential waistline reduction level usually comes across its middle. They access for the liposuction is the Dimples of Venus marks on the lower back which in some patients are very accentuated.The location of the incisions for the internal tissue removals is placed to the side of the back located over rib #11. The incision length is 4cms.

 Once the incision is made dissection is carried down to the latissimus dorsi muscle which is horizontally transected from its lateral border inward 5 to 6 cms. Then the posterior serratus muscle is opened over each rib beginning with the lowest rib #12. Ribs #11 and #12 are identified with a severe downward angulation which is only rarely showed by anatomic pictures or models. The outer portions of ribs #11 and #12 are removed of which rib #11 is by far the longest. Rib #11 impacts waistline support more than any other rib removed.
Once the incision is made dissection is carried down to the latissimus dorsi muscle which is horizontally transected from its lateral border inward 5 to 6 cms. Then the posterior serratus muscle is opened over each rib beginning with the lowest rib #12. Ribs #11 and #12 are identified with a severe downward angulation which is only rarely showed by anatomic pictures or models. The outer portions of ribs #11 and #12 are removed of which rib #11 is by far the longest. Rib #11 impacts waistline support more than any other rib removed.

 Treating rib #10 is the most misunderstood of those removed because of its different anatomy. It does not typically angulate as far downward as ribs #11 and #12 because it wraps around the upper waistline to attach to the subcostal cartilaginous ribcage. Thus it does not have a free floating end and does not directly impact the waistline as much as the lower two ribs. Options are to either remove a bony portion of the rib and disarticulate it from the cartilaginous junction or remove a 5 cm length of the bony rib and have the ‘bridge’ collapse given its proximal and distal attachments. (rib collapsing technique)
Treating rib #10 is the most misunderstood of those removed because of its different anatomy. It does not typically angulate as far downward as ribs #11 and #12 because it wraps around the upper waistline to attach to the subcostal cartilaginous ribcage. Thus it does not have a free floating end and does not directly impact the waistline as much as the lower two ribs. Options are to either remove a bony portion of the rib and disarticulate it from the cartilaginous junction or remove a 5 cm length of the bony rib and have the ‘bridge’ collapse given its proximal and distal attachments. (rib collapsing technique)
The posterior serratus muscle is closed over each the removed rib spaces with long-acting local anesthetic-soaked foam sponges replacing the bony rib. This provides an intercostal block for postoperative pain control. The split latissimus dorsi has wedges of muscle removed both above and below the cut line to reshape the lateral border of the muscle for an additive waistline reduction effect.
 While rib removal surgery does indeed remove rib bone which causes some inward waistline collapse, that trunk contouring effect is enhanced by the addition of fat and muscle removals as well.
While rib removal surgery does indeed remove rib bone which causes some inward waistline collapse, that trunk contouring effect is enhanced by the addition of fat and muscle removals as well.
Dr. Barry Eppley
Indianapolis, Indiana