


Clefts of the orofacial region are one of the most common congenital facial deformities. While not frequent by the numbers (more or less 1:1,000 births) they are still high in the list of potential facial birth defects. In the state of Indiana, for example, where about 80,000 births occur per year, almost one hundred new facial cleft cases present for care each year.
 Orofacial clefts occur in wide range of presentations involving variable splits of the upper lip, upper jaw and palate. They can occur on one side (unilateral) or both sides. (bilateral) Potentially there are dozens of possible combinations of lip and palate involvement. The simplest, however, is the unilateral incomplete cleft lip. It presents as an incomplete split of the lower half of one side of the upper lip. Sometimes it is just a notch in the lip vermilion (pink part) or can almost extend all the way up to the nostril base. There is no involvement of the palate and the upper jaw (alveolus) may or may not have a notch in it based on the extent of the partial lip split.
Orofacial clefts occur in wide range of presentations involving variable splits of the upper lip, upper jaw and palate. They can occur on one side (unilateral) or both sides. (bilateral) Potentially there are dozens of possible combinations of lip and palate involvement. The simplest, however, is the unilateral incomplete cleft lip. It presents as an incomplete split of the lower half of one side of the upper lip. Sometimes it is just a notch in the lip vermilion (pink part) or can almost extend all the way up to the nostril base. There is no involvement of the palate and the upper jaw (alveolus) may or may not have a notch in it based on the extent of the partial lip split.
In the repair of the incomplete cleft lip this is usually undertaken between 3 to 6 months after birth. While there is no pressing medical need to do so (from a feeding standpoint) it still should be done at the timing of all more complete cleft lip repairs. Getting the orbicularis muscle in continuity as early as possible in life is always beneficial.
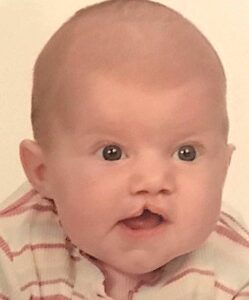
 Like all cleft repairs, in which a lot of facial growth is going to occur after an early repair, the long term outcome is always of great interest. How does the cleft repair look as an adult? Can the patient be recognized for having had a cleft? What type of adult has this little baby with the cleft lip become? While very long term followups are not actually common to the plastic surgeon who performed the repair, every great now and then a patient from a long time ago provides some followup. Here is such a case who generously provided an 18 year followup of her outcome as she graduated from high school and is moving on to college.
Like all cleft repairs, in which a lot of facial growth is going to occur after an early repair, the long term outcome is always of great interest. How does the cleft repair look as an adult? Can the patient be recognized for having had a cleft? What type of adult has this little baby with the cleft lip become? While very long term followups are not actually common to the plastic surgeon who performed the repair, every great now and then a patient from a long time ago provides some followup. Here is such a case who generously provided an 18 year followup of her outcome as she graduated from high school and is moving on to college.
The caveat to this story, and one that I would tell every primary cleft lip patient, is that the vast majority will eventually require a lip revision as the effects of expanding facial growth takes their effects on the initial repair. Such was the case here as a lip revision was performed later as an older child. But in the end her long term outcome demonstrates that the unexpected finding at birth can lead to a very normal facial appearance in the long term..
Dr. Barry Eppley
Indianapolis, Indiana