

The tongue evokes a lot of different reactions from people because of its appearance, location and use in various gestures. While unusual in appearance and movements, its importance in oral function can not be underestimated. It has numerous roles in eating, speech and oral hygiene. It is truly a multifunctional body organ.
The tongue is unique because it is a completely muscular structure that lies within an easily accessible body cavity. If one so desires it can protrude outside the body cavity to perform other functions as well. While the tongue lies both within the oral and pharyngeal cavities it consists mainly of eight pairs of muscle, some of which are attached to bone while other bundles of the muscle are not. Only the very top of the tongue (dorsum) is not muscle and is covered with various taste buds.
From a plastic surgery standpoint the muscular structure of the tongue can serve as a very good pedicled tissue flap for small defect reconstruction. Its rich blood supply from the muscle ensures a well vascularized flap even if made very thin. But because its flap length is rather short, it is only useful in several specific intraoral indications.
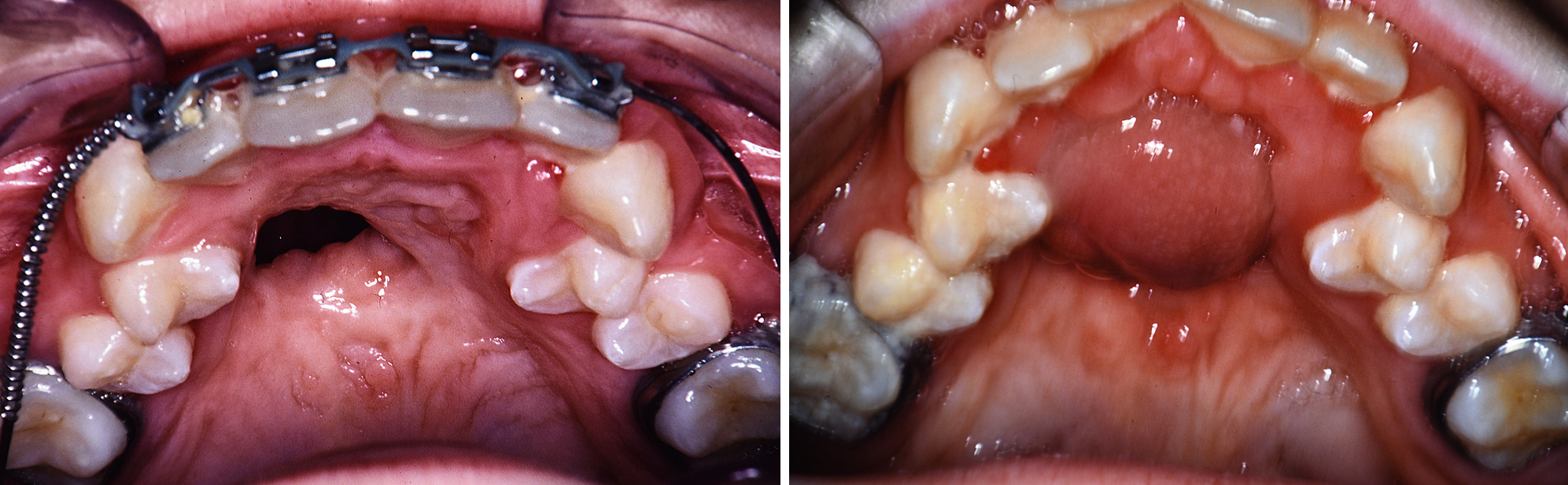
Once of the most common indications for a tongue flap is in cleft palate fistula repair. Particularly in bilateral cleft lip and palate deformities an anterior fistula behind the front teeth is not rare. Trying to close an anterior palate fistula is very difficult using local tissue because it is tight and scarred. In small fistulas local tissue flaps may be successful. But in larger palatal fistulas tissue must be brought in for coverage and this is ideal for the use of a tongue flap.
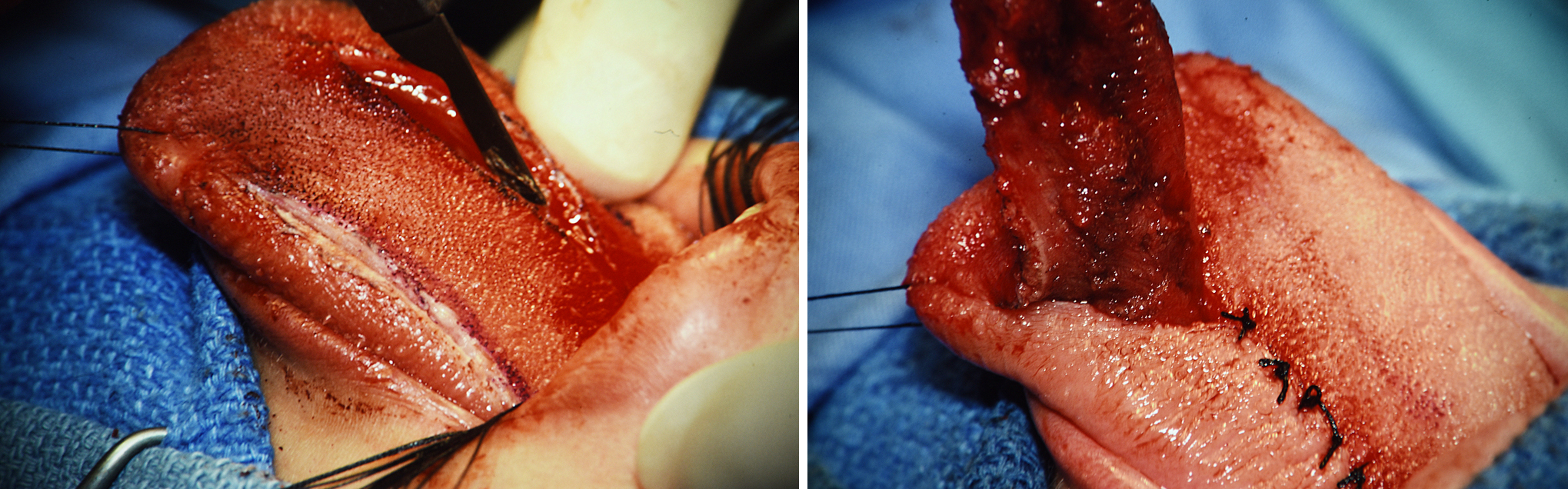 Most tongue flaps are raised with anterior base from back to front. It is best to leave at least a 3 cm wide base and make the flap almost a centimeter thick. It should start just in front of the circumvallate papillae to get the longest length possible. Due to the large lingual veins buried inside the tongue one does not want to go too deep either. The flap is folded back and its raw undersurface sewn around the perimeter over the fistula whose edges have been opened.
Most tongue flaps are raised with anterior base from back to front. It is best to leave at least a 3 cm wide base and make the flap almost a centimeter thick. It should start just in front of the circumvallate papillae to get the longest length possible. Due to the large lingual veins buried inside the tongue one does not want to go too deep either. The flap is folded back and its raw undersurface sewn around the perimeter over the fistula whose edges have been opened.
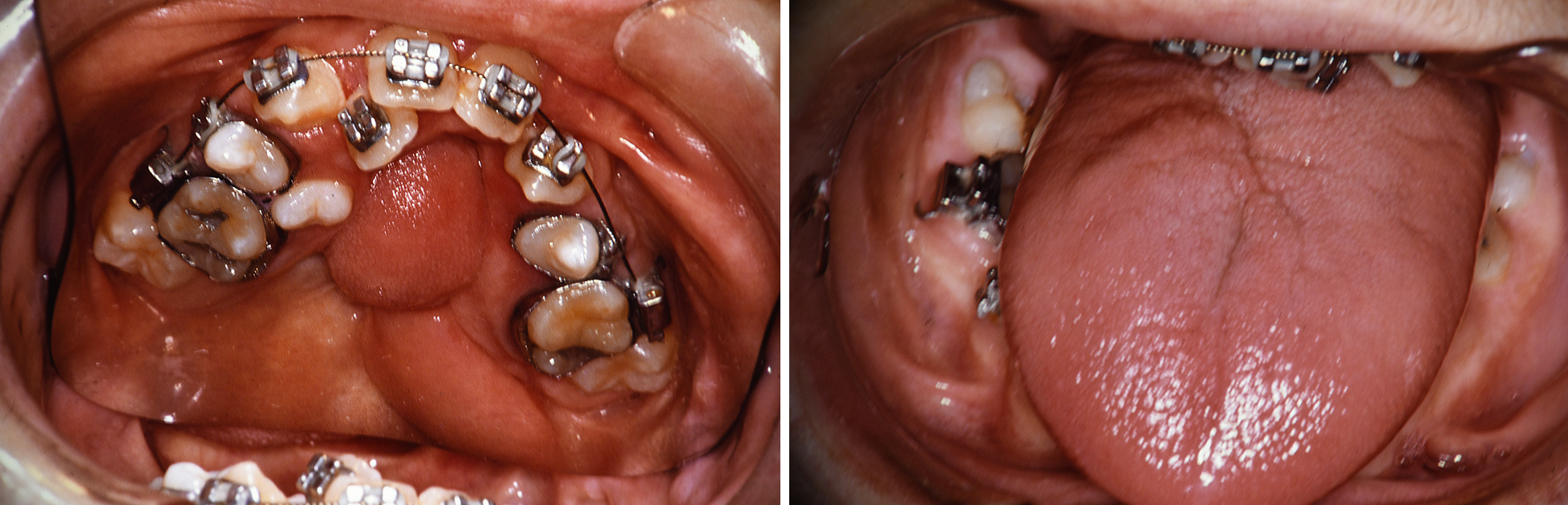 Tongue flaps are left in place for about 3 weeks so it can acquire a blood supply into the end of the flap. Thereafter the flap is separated from the tongue and the tongue donor site and the palatal fistula site closed. This leaves a bulk of thick tongue tissue over the fistula site but ensures a competent closure of it. Some of the muscle will shrink over time, since it is no longer functioning as a muscle, and if still too bulky can be thinned out later. The donor site of the tongue heals very well and usually without much deformity because of a midline harvest.
Tongue flaps are left in place for about 3 weeks so it can acquire a blood supply into the end of the flap. Thereafter the flap is separated from the tongue and the tongue donor site and the palatal fistula site closed. This leaves a bulk of thick tongue tissue over the fistula site but ensures a competent closure of it. Some of the muscle will shrink over time, since it is no longer functioning as a muscle, and if still too bulky can be thinned out later. The donor site of the tongue heals very well and usually without much deformity because of a midline harvest.
Dr. Barry Eppley
Indianapolis Indiana