

Introduction
Torso narrowing by rib removal is a skeletal-based body contouring procedure designed to permanently reduce waist width by altering the lower rib cage. It is indicated only for a small, carefully selected subset of patients.
 What Rib Removal Actually Means
What Rib Removal Actually Means
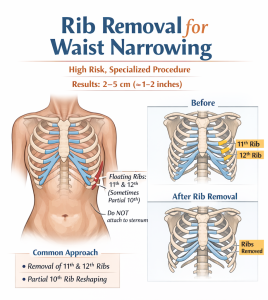
- The procedure most commonly targets the 11th and 12th ribs, also known as the floating ribs.
- These ribs do not attach to the sternum.
- Rib 10 has more recently been addressed through either subtotal removal or a “bridge-collapsing” technique.
- These lower ribs contribute significantly to the lateral flare of the lower torso.
- To maximize the visible effect of skeletal narrowing, lateral reduction of the latissimus dorsi muscle is now routinely performed in conjunction with rib removal.
How Rib Removal Achieves Waist Reduction
- Removal or shortening of the ribs reduces the bony width of the lower torso.
- This allows the waist to taper inward at the skeletal level.
- When only ribs 11 and 12 are treated, the degree of torso narrowing is limited.
- Results are permanent.
- The change is typically moderate in most patients, often averaging 2–5 cm per side, depending on individual anatomy.
Surgical Approaches
- Posterior (back) or vertical lateral back incisions are used.
- Partial rib resection is performed rather than complete rib removal.
- Liposuction may be added if flank fat is present to enhance the visible result.
- The procedure requires general anesthesia.
Who Is a Good Candidate
Ideal candidates are patients at an appropriate body weight for their height who have:
- Minimal waist and flank fat
- Prominent lower rib flare
- Inadequate results from prior liposuction or abdominoplasty
- Stable body weight
- A clear understanding that the achieved result represents the maximum possible skeletal change
Who Is Not a Good Candidate
Patients with the following characteristics are poor candidates:
- Significant abdominal or flank fat
- No prior attempt at traditional surgical or non-surgical body contouring
- Unrealistic expectations
Rib removal is not a first-line waist-narrowing procedure. It should only be considered after fat and soft-tissue solutions have been exhausted and when skeletal anatomy—not adiposity—is the primary limiting factor. Even then, the torso-narrowing effect remains inherently limited.
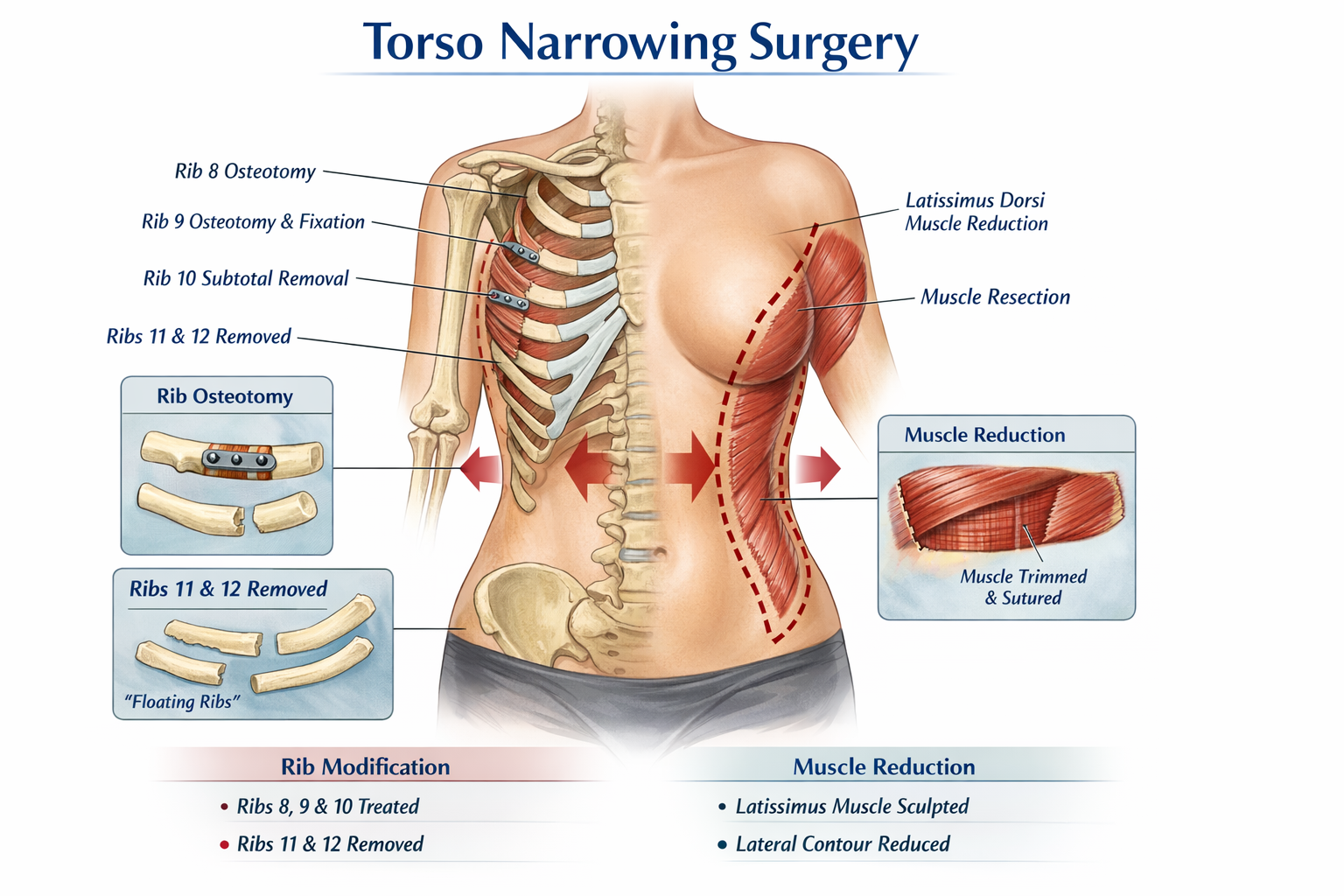
How Torso Narrowing Surgery Differs from Traditional Rib Removal
 Structural torso narrowing is an extension of conventional rib removal surgery. To achieve greater narrowing of the lower torso, ribs 8, 9, and 10 are also addressed:
Structural torso narrowing is an extension of conventional rib removal surgery. To achieve greater narrowing of the lower torso, ribs 8, 9, and 10 are also addressed:
- Rib 10: subtotal removal
- Rib 9: osteotomy with reduction
- Rib 8: osteotomy reduction or cortical shaving
These rib modifications are combined with a longer and wider resection of the latissimus dorsi muscle to further reduce lateral torso width.
Case Study
This patient desired a narrower torso after achieving maximal reasonable weight loss. The waistline had minimal subcutaneous fat, and the lower ribs (8 through 11) were highly palpable (rib 12 is almost never palpable in any patient).

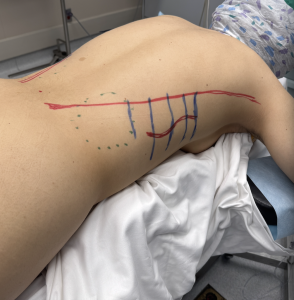
 An oblique red line was marked from the upper buttocks to the axilla to guide the proximal rib cuts. A wavy lateral back incision was planned and marked between the levels of ribs 8 and 11. The patient expressed no concern regarding scarring and prioritized maximal surgical effect.
An oblique red line was marked from the upper buttocks to the axilla to guide the proximal rib cuts. A wavy lateral back incision was planned and marked between the levels of ribs 8 and 11. The patient expressed no concern regarding scarring and prioritized maximal surgical effect.





 Under general anesthesia, the patient was positioned prone. The ribs were accessed by splitting the thick latissimus dorsi muscle, exposing the serratus muscle and underlying ribs.
Under general anesthesia, the patient was positioned prone. The ribs were accessed by splitting the thick latissimus dorsi muscle, exposing the serratus muscle and underlying ribs.
- Rib 12: a 3 cm segment, including its cartilaginous tip, was removed.
- Rib 11: a 14 cm segment was excised.
- Rib 10: a 15 cm segment was removed, extending to the anterior subcostal attachment.
- Rib 9: treated with a 1.5 cm osteotomy; the distal segment was mobilized and secured to the proximal segment using plate-and-screw fixation.
- Rib 8: treated by shaving the outer cortical surface.



 The latissimus dorsi muscle was reduced in width by excising a 4 cm-wide segment over a 30 cm length, extending beyond both the upper and lower ends of the incision. Removal along the muscle split allowed the lateral border to be advanced inward and sutured to the medial muscle edge, maintaining a smooth contour while achieving significant inward repositioning.
The latissimus dorsi muscle was reduced in width by excising a 4 cm-wide segment over a 30 cm length, extending beyond both the upper and lower ends of the incision. Removal along the muscle split allowed the lateral border to be advanced inward and sutured to the medial muscle edge, maintaining a smooth contour while achieving significant inward repositioning.

 Following drain placement and closure, the torso-narrowing effect was clearly visible from the posterior view.
Following drain placement and closure, the torso-narrowing effect was clearly visible from the posterior view.
 In the oblique view, the incision line had shifted closer to the preoperatively marked red reference line, further demonstrating the degree of narrowing achieved.
In the oblique view, the incision line had shifted closer to the preoperatively marked red reference line, further demonstrating the degree of narrowing achieved.
Discussion
The evolution of ribcage modification from the floating ribs upward to the false ribs is based on an understanding of their differing anatomy.
- Ribs 11 and 12 can safely undergo removal or fracture techniques because their distal ends are unattached and lie below the level of the lung pleura.
- Rib 11 contributes more to waist narrowing than rib 12 due to its greater length.
- Rib 10 plays a critical role in lateral torso width because it wraps anteriorly to the subcostal margin. Although it lacks a rigid articulation with rib 9, its fibrous attachment renders its distal end relatively immobile. Subtotal removal of its arced portion is therefore effective, while fracture techniques are less reliable.
- Manipulation of rib 10 requires heightened caution, as the pleura may lie close to or adhere to the posterior rib surface.
For ribs above this level, full removal is not advisable. Fracture techniques are ineffective due to rigid proximal and distal attachments. Osteotomy techniques, however, have proven useful by removing a segment of the lateral arc and approximating the cut ends. Because plate fixation requires perpendicular access, longer incisions are necessary, as demonstrated in this case. The same principle applies to rib 8 osteotomies.
An often-overlooked contributor to waist width is the lateral border of the latissimus dorsi muscle. This broad muscle extends laterally beyond the ribs from its humeral attachment down to the iliac crest. Resection-based inward repositioning of the muscle complements rib modification by further reducing lateral torso width.
Key Points
- Torso narrowing surgery extends traditional rib removal by addressing higher rib levels and performing longer latissimus dorsi resections.
- The procedure requires a longer lateral vertical incision compared to standard rib removal surgery.
- Torso narrowing goals are tailored to transfeminine body contouring objectives.
- The upper limit of ribcage narrowing via osteotomy remains unknown, but progressively longer incisions are required at higher levels.
Barry Eppley, MD, DMD
World-Renowned Plastic Surgeon