

Temporal reduction to decrease side-of-head convexity is fundamentally about flattening the outward bulge in the temporal region (particularly above the ears). This convexity is most commonly caused by a thick temporalis muscle rather than the underlying bone.
Core Concept
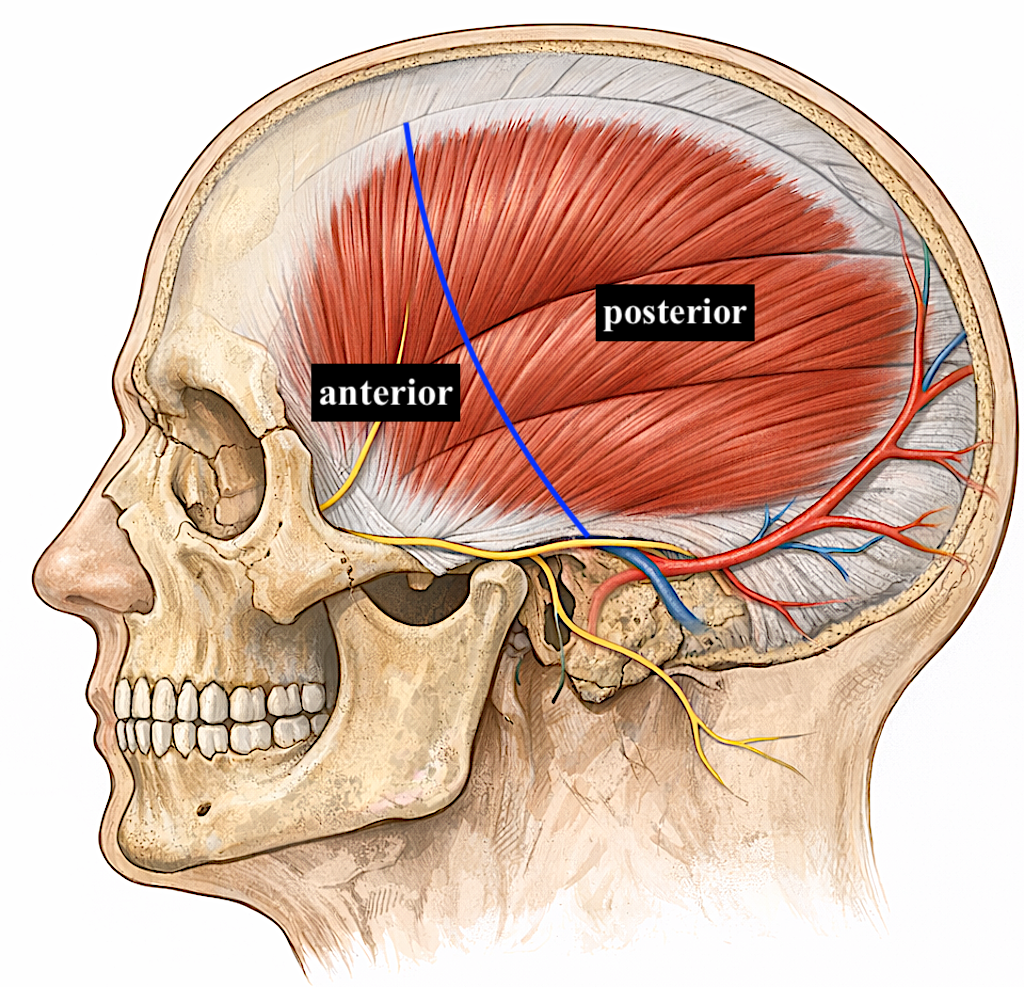
The convex (bulging) shape of the lateral head is largely due to the thickness and projection of the temporalis muscle. The underlying skull in this area is typically not excessively wide, so bone reduction alone has limited impact. Effective contour change, therefore, comes from soft tissue (muscle) reduction or removal.
Surgical Temporalis Muscle Reduction (Definitive Approach)
Goal:
To permanently flatten the side of the head.
Technique (high-level):
- Access through a small incision behind the ear (postauricular approach)
- Total resection of the posterior temporalis muscle
- Preservation of function by maintaining the anterior muscle (more critical for mastication)
Why target the posterior muscle?
- It contributes most to visible width and convexity
- It has less functional importance than the anterior portion
Effect:
- Reduced outward projection
- Straighter or slightly concave side profile
- Narrower upper facial and head appearance
Large Wide Heads / Global Temporal Muscle Enlargement
Less commonly, the entire temporalis muscle is enlarged, creating an extremely wide head shape. In these cases, the muscle may protrude beyond the bony temporal line, including the anterior portion.
 In such patients, the anterior temporal region can exhibit greater convexity than the posterior region. As a result, isolated posterior muscle removal is insufficient to achieve adequate narrowing.
In such patients, the anterior temporal region can exhibit greater convexity than the posterior region. As a result, isolated posterior muscle removal is insufficient to achieve adequate narrowing.
Case Example
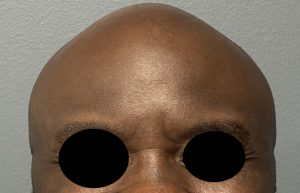
 This male patient had been bothered for most of his life by a very wide head shape. His head circumference measured 64.5 cm (normal male range: 54–57 cm). He was unable to wear standard hats and required specially designed glasses with convex ear extensions. He also had a history of bruxism and temporal headaches.
This male patient had been bothered for most of his life by a very wide head shape. His head circumference measured 64.5 cm (normal male range: 54–57 cm). He was unable to wear standard hats and required specially designed glasses with convex ear extensions. He also had a history of bruxism and temporal headaches.
 A 2D CT scan demonstrated significant enlargement of the temporalis muscle, including a prominent anterior component.
A 2D CT scan demonstrated significant enlargement of the temporalis muscle, including a prominent anterior component.
I
 n surgery, the temporalis muscle thickness at the level of the upper ear measured 15 mm. A combined approach was performed through postauricular incisions, consisting of:
n surgery, the temporalis muscle thickness at the level of the upper ear measured 15 mm. A combined approach was performed through postauricular incisions, consisting of:
- Posterior temporalis muscle removal
- Anterior temporalis muscle transposition
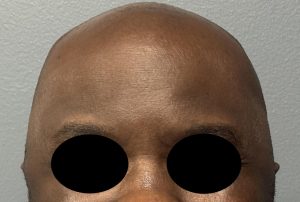
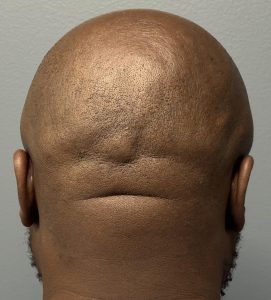
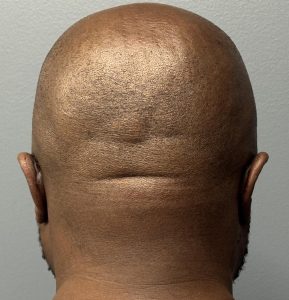 Postoperative results (day one) showed a clear reduction in temporal fullness. The contour improvement was more evident in the frontal view than in the posterior view, reflecting the greater anterior muscle thickness.
Postoperative results (day one) showed a clear reduction in temporal fullness. The contour improvement was more evident in the frontal view than in the posterior view, reflecting the greater anterior muscle thickness.
Discussion
![]() Anterior temporalis muscle transposition for aesthetic head narrowing involves repositioning part of the anterior muscle rather than completely excising it. This approach reduces anterior temporal convexity (bitemporal fullness) and creates a narrower head contour.
Anterior temporalis muscle transposition for aesthetic head narrowing involves repositioning part of the anterior muscle rather than completely excising it. This approach reduces anterior temporal convexity (bitemporal fullness) and creates a narrower head contour.
The anterior temporal region presents unique challenges:
- It is highly visible
- Surgical access is limited via a postauricular incision
- Complete muscle removal is generally not feasible
To address this, a technique has been developed involving:
- Partial anterior muscle reduction/release
- Posterior and/or inferior transposition
In contrast, posterior temporal width reduction is more amenable to direct muscle excision.
From an anatomical standpoint, this approach is logical. The temporalis is a broad, fan-shaped masticatory muscle with a segmental blood supply from:
- Anterior and posterior deep temporal arteries
- Contributions from the middle temporal artery
Any transposition must preserve adequate vascularized muscle and avoid visible contour deformities, particularly in the hairless anterior temporal fossa.
Tradeoffs and Considerations
The primary tradeoff is that reducing or repositioning the anterior temporalis to narrow the head can lead to:
- Temporal hollowing
- Contour irregularities
- Chewing weakness
- Dynamic deformities
These risks are well documented in reconstructive literature. Traditional temporalis transposition can result in donor-site hollowing, and neurosurgical studies have explored anterior muscle rotation techniques specifically to prevent postoperative temporal defects.
Practical Summary
- Goal: Reduce visible anterior side-of-head fullness
- Mechanism: Partial anterior temporalis release with posterior/inferior redistribution (rather than full excision)
- Indication: Only permanent method to reduce anterior temporal muscle fullness
- Challenge: High visibility of the region—overcorrection can quickly lead to hollowing or asymmetry
Final Perspective
There is limited peer-reviewed aesthetic literature supporting this procedure as a routine cosmetic operation. Most published data relates to reconstructive temporalis transposition or correction of temporal hollowing rather than aesthetic head narrowing.
Thus, while the anatomical rationale is sound, this remains a niche, technique-sensitive procedure in which surgeon experience, judgment, and careful patient selection are critical.
Dr. Barry Eppley
Plastic Surgeon